Download
1 / 20
200 likes | 854 Views
British Guideline on the Management of Asthma. Aims. Review of current SIGN/BTS guidelines Diagnosing Asthma Stepwise management of Asthma Managing Acute Asthma When to admit. Age Groups. Children Adults. Diagnostic Algorithms. Clinical features

E N D
Aims • Review of current SIGN/BTS guidelines • Diagnosing Asthma • Stepwise management of Asthma • Managing Acute Asthma • When to admit
Age Groups • Children • Adults
Diagnostic Algorithms • Clinical features • Increase/decrease the probability of Asthma • Diagnostic probability • Low, intermediate and high.
Increase Wheeze, cough, shortness of breath, tight chest. Worse at night/morning Triggers Exercise,allergen,cold air, drugs Atopy FH asthma/atopy Widespread wheeze Response to treatment Unexplained low FEV1 or eosinophilia Decrease No interval symptoms Cough only Moist cough Hyperventilation symptom Normal examination Normal PF/spirometry No response to Rx Cardiac disease Voice disturbance Significant smoking history Clinical features & Probability
Management • Non-pharmacological • Breast feeding • Avoidance of tobacco smoke • Weight reduction • Pharmacological
Pharmacological Management • Aim for complete control • No daytime symptoms, no night time awakening, no need for rescue meds, no exacerbations, normal activity, normal lung function. • Stepwise approach • Start at most appropriate step • Early control • Maintain by stepping up or down
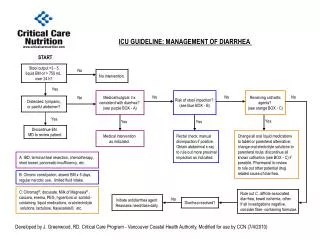
Management of Acute Asthma • Assessment • Clinical features • PEF • Pulse oximetry • Blood gases (ABG) • Chest X-ray • Not routine • Suspected pneumothorax, consolidation, life threatening, failure to respond, requiring ventilation
Management of Acute Asthma • Moderate • PEFR >50-75% • No severe features • Severe • PEFR 33-50% • RR ≥ 25 (adult), >30 (>5yrs), >40 (2-5yrs) • HR ≥ 110 (adult), >125 (>5yrs), >140 (2-5yrs) • Unable to complete sentences or feed • Life threatening • PEFR <33% • SpO2 <92% • Silent chest, cyanosis, exhaustion, altered consciousness
Management of Acute Asthma • Oxygen • Hypoxic patients – aim 94-98% • Drive nebulisers with oxygen • 2 agonist bronchodilators • As early as possible • Consider continuous nebulisers if poor initial response • Oral steroids • Ipratropium bromide • IV magnesium sulphate • Poor response to 2 agonist or life threatening • IV salbutamol/aminophylline - Paediatrics
Admission criteria - Adults • Life threatening • Immediately • Severe • If any features of severe attack after initial treatment
Admission criteria - Children • Severe of life threatening • Immediately • Moderate • No improvement after 10 puffs of 2 agonist
Difficult Asthma • Persistent symptoms or frequent exacerbations despite step 4 or 5 • Confirm diagnosis • Consider poor compliance • Consider psychosocial assessment
Conclusion • Asthma is frequently under treated • Use current guidelines to aid diagnosis and help in acute and chronic management • If patients are not responding as you would expect • Is the diagnosis right? • Are they taking the appropriate medication? • Are psychological or social factors hindering management?