Download
1 / 20
200 likes | 360 Views
Scope Guideline for Asthma. นศ.ภ.ณัฐพร นุกูลกิจ 483150013-8 ชั้นปีที่ 5 มหาวิทยาลัยขอนแก่น รายวิชา Ambulatory care ( ผลัดที่ 2/2552). Asthma. Symptoms. Loss work. OPD visit. ER visit. Admission. Dead. Asthma admission in Thailand (excluding Bangkok).

E N D
Scope Guideline for Asthma นศ.ภ.ณัฐพร นุกูลกิจ 483150013-8 ชั้นปีที่ 5 มหาวิทยาลัยขอนแก่น รายวิชา Ambulatory care (ผลัดที่ 2/2552)
Asthma Symptoms Loss work OPD visit ER visit Admission Dead
Asthma admission in Thailand (excluding Bangkok) Health Information Division, Bureau of Health Policy and Planing
Burden in Thailand* • Cost of health care (exclude testing) • 990 million Bahts in 2546 • 1,087 million Bahts in 2547 *Association of Allergy & Immunology of Thailand
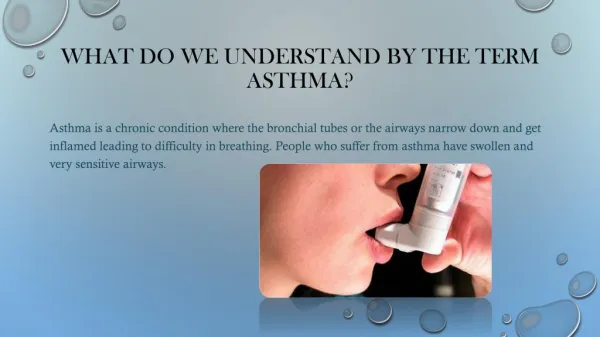
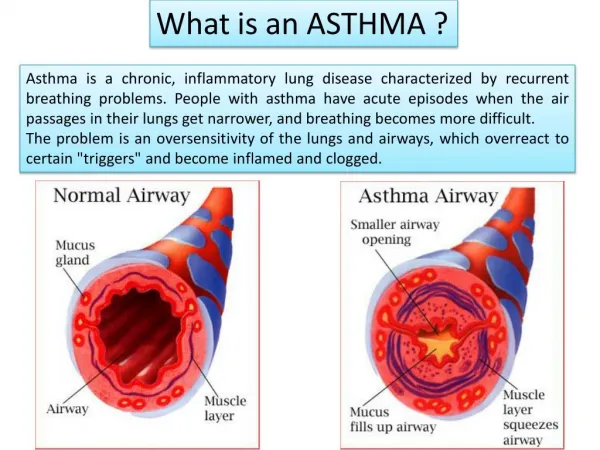
Asthma • Reversible inflammation & obstruction • Intermittent attacks • Sudden onset • Varies from person to person • Severity can vary from shortness of breath to death
Asthma Diagnosis • History and patterns of symptoms • Physical examination • Measurements of lung function
New • 1995 • 2002 • 2004 • 2006 • 2007 • 2008
Changing concept in asthma treatment short-acting b2-agonists Combination Inh corticosteroid Bronchospasm Inflammation Airway Hyperresponsiveness Remodelling 1980 1985 1990 1995 2000 1975
GINA 1995-2005 • Severity classification • Stepwise treatment according to severity
Classification of Asthma Severity (GINA 1995)
Treatment in GINA 2002 Severe Persistent Moderate persistent Mild persistent Intermittent ß2 prn Inhsteroids LABA
1995 2002 GINA 1995-2002 • Day symptoms • Night symptoms • Reliever • PEFR • Exacerbation • Limitationof activity Aim: Asthma control 4. Severe persistent Asthma severity 3. Moderate persistent 2. Mild persistent 1. Intermittent 4. SABA+ICS+LABA+pred 3. SABA+ICS+LABA Treatment 2. SABA +ICS 1. SABA prn
Outcome: asthma control Outcome: best possible results Controller High-dose inhaled corticosteroid + long-actinginhaled 2-agonist plus if needed Theophylline-SR Leukotriene modifier Oral 2-agonist Oral corticosteroid Anti-IgE Controller Low-to-medium-dose inhaledcorticosteroid +long-acting inhaled 2-agonist (theophylline, leukotriene modifier,oral 2-agonist) Controller Controller Low-doseinhaledcorticosteroid(theophylline, leukotriene modifier, cromolyn) None Reliever: rapid-acting inhaled β2-agonist prn Step 3Moderatepersistent Step 4Severe persistent Step 1Intermittent Step 2Mild persistent Treatment in GINA 2004 Global Initiative for Asthma (2004 update published 2005)
2006 Assess asthma control Adjust treatments according to level of asthma control
Revised 2006 Asthma Management and Prevention Program: Five Components 1. Develop Patient/Doctor Partnership 2. Identify and Reduce Exposure to Risk Factors 3. Assess, Treat and Monitor Asthma 4. Manage Asthma Exacerbations 5. Special Considerations: AR, AS
Levels of Asthma Control: GINA 2006 * Any exacerbation should prompt review of maintenance treatment to ensure that it is adequate. †By definition, an exacerbation in any week makes that an uncontrolled asthma week. ‡ Lung function is not a reliable test for children 5 years and younger.
Management approach based on control Reduce Increase GINA 2006
Controller Options GINA 2006
2006 GINA 2006 • Day symptoms • Night symptoms • Reliever • PEFR • Exacerbation • Limitationof activity Assessing asthma control • Controlled • Partly controlled • Uncontrolled Treating to achieve asthma control • B2-agonist prn • ICS or LTM • ICS (low dose) + LABA • ICS (high dose) + LABA, LTM, theophylline • ICS (high dose) + LABA + prednisolone Monitoring to maintain control In treatment-naïve patients started at Step 2. In very symptomatic (uncontrolled) started at Step 3.