Download
1 / 30
350 likes | 747 Views
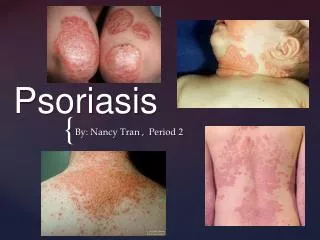
Psoriasis. Definition. Chronic plaque psoriasis (psoriasis vulgaris) is a chronic inflammatory skin disease characterised by well demarcated erythematous scaly patches on the extensor surfaces of the body and scalp Lesions may itch, sting and occasionally bleed

E N D
Definition • Chronic plaque psoriasis (psoriasis vulgaris) is a chronic inflammatory skin disease characterised by well demarcated erythematous scaly patches on the extensor surfaces of the body and scalp • Lesions may itch, sting and occasionally bleed • Dystrophic nail changes are found in > 1/3 • Psoriatic arthropathy occurs in 1->10% • Condition waxes and wanes with wide variations between individuals • Other types – guttate, inverse, pustular, erythrodermic
Epidemiology of psoriasis • Affects 1.5% in UK • Ethnic variation • Rare in Japan and China • M = F • Bimodal age distribution • Commonest between 10 and 20 years and around 50 years • Many cases mild • Can be very stigmatising • 5% get episodes of severe disease • Precipitants / aggravants • Alcohol, NSAIDs, B blockers, Lithium, antimalarials
Pathology • Rapid proliferation of keratinocytes (x7 normal rate) causes acanthosis = thickening of epidermis due to increased numbers of acanthocytes (prickle cells) • Incomplete differentiation and maturation causes cells to be shed in abnormally large clumps • Dilatation and elongation of capillaries – apparent at surface • Infiltration of dermis and epidermis by inflammatory cells causes microabscesses and micropustules : pustular psoriasis • Cause unknown. Though to be autoimmune – genetic influence – 30% have a relative with the condition
Chronic plaque psoriasis • Commonest type • Scaly erythematous plaques – red, white-silver scale, well demarcated • Itch common, pain unusual • Symmetrical distribution • Common sites • Scalp, elbows, knees, shins and sacrum • Nail involvement common • Koebner’s phenomenon useful pointer • Activity varies over months to years, remission common, sometimes induced by treatment
Guttate psoriasis • Acute eruption of small plaques (typically 1cm) over trunk and limbs • Triggered by URTI – particularly streptococcal sore throat
Palmopustular psoriasis • More often affects women • Strong correlation with smoking • Chronic relapsing course, difficult to treat (often needs systemic treatment) • Can be painful • When occurs on its own, difficult to distinguish from eczema
Nail psoriasis • Pitting and onycholysis, subungal hyperkeratosis • Can occur in isolation
Flexural and genital psoriasis • Looks different, not always scaly • Exudation prominent
Severe types / manifestations of psoriasis • Generalised pustular psoriasis • Often erupts suddenly. Life-threatening • Some cases associated with withdrawal of topical or systemic steroids • Sheets of small pustules merge • Associated pyrexia and systemic illness • Sepicaemia, shock, dehydration can occur • Erythrodermic psoriasis • Usually seen in neglected or poorly controlled severe psoriasis • Severe erythema and scaling over entire body surface • Psoriatic arthritis
General assessment – disease severity • Patient satisfaction • Disease related quality of life • Surface area covered • <5% is mild – one palm area = 1% body area • 5-20% is moderate – often requires hospital intervention, usually topical / oral regimen with UV light therapy • >20% is severe – requires systemic therapy
Many therapies Community based Hospital led Phototherapy Methotrexate Oral retinoids Cyclosporin Hydroxyurea Azathioprine Systemic steroids TNF-alpha drugs T-cell drugs – efalizumab, alefacept • Emollients • Topical coal tar • Topical dithranol • Topical vitamin D and analogues • Topical corticosteroids • Topical retinoids • Plus combinations
British association of Dermatologists recommendations • Emollients soften scaling and reduce irritation • For localised plaque psoriasis one or more of the following can be used : • Tar based cream or tar/corticosteroid mixture • Moderate potency topical corticosteroid eg eumovate • Stronger agents can be used on the palms and soles or on the scalp • Vitamin D analogue • Calcipotriol with betamethasone dipropionate combination product • Vitamin A analogue (tazarotene) • Dithranol preparation • Use a keratolytic agent (eg 5% salicylic acid in emulsifying ointment) first when there is significant scaling or other treatments fail
Topical tar • Newer ‘cleaner’ creams more acceptable – up to 10% coal tar • Stronger ‘crude’ preparations are usually part of hospital based treatment • Shampoo particularly useful • Traditionally been used combined with UVB therapy (Goeckermann treatment) • Trend towards alternating applications with topical steroids • Expensive now! • Tried and tested (100 years plus) • Smelly • Can stain clothing and skin • Safety concerns (no long term evidence of increased cancer risk)
Dithranol • Best suited to largeish, well-defined plaques • Not for flexures • Start with low strength and build up, from 0.1 up to 3% • Miconal is a newer product claiming to release dithranol at body temp (and causes less staining) • Apply for 30 mins and wash off )vary between 5 and 60 mins • Tried and tested (50y) • Cheap • Not easy to use • Wear gloves or wash off hands carefully • Irritating and can ‘burn’ healthy skin • Stains (brown/purple) – skin, clothes, bath etc
Vitamin D and analogues • Calcipotriol • OD or BD • Irritation – redness, soreness and pruritis common (20%) • Not to be used on face or flexures • No more than 100g per week (risk of hypercalcaemia) • Calcitriol • BD • Max 30g daily • Not children • Can be used on creases and face • Tacalcitol • Once daily • Not children • Max 10g per day • Can be used on creases and face
Topical steroids • Effective in short term, relatively cheap • Generally liked by patients – not smelly / messy • Early improvement not sustained • Do not use more than 4 weeks • Problem is rebound effects or aggrevation /instability • Mild steroid useful for creases and face • Potent steroid often useful as initial treatment for scalp, hands and feet • Can be used with dithranol, coal tar, vitamin D and analogues • Dovobet allows steroid and calcipotriol application at the same time
Dovobet – betamethasone 0.05% with calcipotriol • OD or BD • Indicated for stable plaque psoriasis (age greater than 18) • Not to be applied to scalp, face, mouth (or eyes) – also avoid creases • Max 4 weeks, max 15g/day, 100g/week • No more than 30% of total body surface
Tazarotene (Zorac) • Indicated for mild to moderate plaque psoriasis affecting up to 10% of skin area • OD up to 12 weeks ; not on face • Not recommended under 18 • Teratogenic – must not be used in pregnancy • Helps regulate abnormal proliferation of keratocytes • Can be quite irritant but is clean and convenient • DTB advise not using first line • Potential for use in combination therapy
Trend is towards combination therapy • All topical therapies have limitations • Irritation, staining, smell, inconvenience etc • Most work through different mechanisms so effects might be additive or synergistic • Potential for combining approaches • Improving therapeutic effects • Minimizing adverse effects
Special sites – skin creases, genitals • Tricky to diagnose and treat • Appearance may not be typical – erythema prominent, scale not evident, may ‘exude’ • Topical corticosteroids often used but avoid high potency – these areas prone to skin atrophy • Use creams rather than ointments • Tacalcitol may be used • Calcipotriol may be too irritant
Scalp • Tends to be visible and stigmatising • Is difficult to manage • Soften thick scale with coconut or arachis oil, can be left on overnight, under shower cap (with salicylic acid, if required) • Remove using combing and shampoo – tar based • Apply coal tar, dithranol, or topical steroid preparation • Newer calcipotriol scalp application is an alternative
Psoriatic arthropathy • 15-20% attending hospital develop inflammatory arthritis • May be <10% in the community • Slight female predominance • Most have pre-existing skin or nail psoriasis (joint inflammation precedes psoriasis in 15% of cases)