Download
1 / 34

E N D
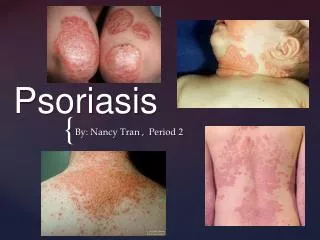
Definition • Psoriasis is a common, chronic, disfiguring, inflammatory and proliferative condition of the skin; in which both genetic and environmental influences play a critical role characterised by red, scaly, sharply demarcated indurated plaques of various sizes, particularly over extensor surfaces and scalp.
Aetiopathogenesis • Genetic predisposition: HLA-B13, B17, and Cw6 • Epidermal hyperproliferation • Antigen driven activation of autoreactive T-cells • Angiogenesis • Multifactorial inheritance • Overexpression of Th1 cytokines such as IL 2, IL 6, IL 8, IL 12, INF - γ, TNF α
Trigger factors • Trauma (Koebner phenomenon): Mechanical, chemical, radiation trauma. • Infections: Streptococcus, HIV • Stress • Alcohol and smoking • Metabolic factors: pregnancy, hypocalcemia • Sunlight: usually beneficial but in some may cause exacerbation
Trigger factors Drugs: Beta-blockers NSAIDS ACE inhibitors Lithium Antimalarials Terbinafine Calcium channel blockers Captopril Withdrawal of corticosteroids
Patient Profile • Sex: Adults (M=F) but in adolescents (F>M) • Age: 2 peak age ranges 1st peak : 16-22 years 2nd peak: 57-60 years • Earlier age of onset: Female sex Positive family history • 3-fold higher risk in siblings of patients with onset before 15 years of age
History • Patients give H/O Prominent itchy, red areas with increased skin scaling and peeling. • New lesions appearing at sites of injury/trauma to the skin (Koebner phenomenon) • Actual clearance of lesions following trauma to the skin (Reverse Koebner phenomenon) • Exacerbation in winter, improvement in summer • Significant joint pain, stiffness, deformity in 10-20%
Morphology • Classical Lesion: Erythematous, round to oval well defined scaly plaques with sharply demarcated borders • Scales: Psoriatic plaques typically have a dry, thin, silvery-white or micaceous scale. • Sites: Elbows, knees, extensors of extremities, scalp & sacral region in a symmetric pattern. Palms/ soles involved commonly
Morphology • Auspitz sign: Removing the scale reveals a smooth, red, glossy membrane with tiny punctate bleeding points • Grattage test: On grattage, characteristic coherence of scales seen as if one scratches a wax candle(‘signe de la tache de bougie)
Morphology • Koebner’s phenomenon Linear distribution of the plaques seen along scratch marks or at sites of trauma • Woronoff‘s ring Psoriatic plaques occasionally appear to be immediately encircled by a paler peripheral zone.
Morphological Types • Chronic plaque psoriasis: plaques with less scaling • Follicular psoriasis: follicular papules. • Linear psoriasis: linear arrangement of plaques • Annular/ figurate psoriasis: ring shaped or other patterns. • Rupoid, elephantine and ostraceous psoriasis
Morphological Types • Guttate psoriasis: Common in children , good prognosis • Pustular psoriasis: Crops of pustules based on erythema • Localised / generalised • Impetigo herpetiformis • Erythrodermic psoriasis: 16-24% of all cases of exfoliative dermatitis
Distributional Variation • Scalp psoriasis • Palmoplantar psoriasis • Nail psoriasis: pitting, onycholysis, subungual hyperkeratosis, or the oil-drop sign. (25-50%) • Mucosal psoriasis • Inverse psoriasis: • spares the typical extensor surfaces • affects intertriginous (i.e, axillae, inguinal folds, inframammary creases) areas with minimal scaling.
Psoriasis in children and in HIV Psoriasis in children: • Plaques not as thick as in adults, less scaly • Diaper area in infants, flexural areas in children • Face involvement more common than in adults Psoriasis in HIV: • Acute onset • Severe flares • Poor prognosis
Psoriatic arthritis • Seen in 5-10% of psoriatic patients • Types: 1. Classic (16%)-DIP joint involvement 2. Oligoarticular (70%) 3. Rheumatoid type(15%) 4. Psoriatic spondylitis (5%) 5. Arthtritismutilans (5%) Contd…
Psoriatic arthritis Associations: • Tenosynovitis • Enthesitis • Osteolysis • New bone formation • Joint fibrosis & ankylosis
Complicated psoriasis • Erythrodermic psoriasis • Generalisedpustular psoriasis • Psoriatic arthritis
Histopathology Skin biopsy findings: • Parakeratosis • Microabscesses of Munro in the horny layer • Absence of granular layer • Regular elongation of rete ridges (camel-foot shaped) • Suprapapillary thinning of st.malphigii • Spongiform pustules of Kogoj • Dilated and tortuous capillaries in dermal papillae • Superficial perivascular inflammatory infiltrate
Differential diagnosis • Nummular eczema • Tineacorporis • Lichen planus • Secondary syphilis • Pityriasisrosea • Drug eruption • Candidiasis • Tineaunguium • Seborrheic dermatitis
Treatment General measures: • Counselling regarding the natural course of the disease • Weigh reduction in obese patients. • Avoidance of trauma or irritating agents. • Reduce intake of alcoholic beverages. • Reduce emotional stress • Sunlight and sea bathing improve psoriasis except in photosensitive
Topical therapy • Emollients: white soft paraffin & liquid paraffin • Corticosteroids: Potent steroids like fluocinoloneacetonide, betamethasonedipropionate or clobetasol propionate • 5-10% Coal tar: for stable but resistant plaques • 0.1-1% dithranol: for few stable, thick, resistant plaques Contd…
Topical therapy • Keratolytics & humectants: as adjuvantseg. Salicylic acid 3-10%, urea 10-20% • Calcipotriene • Tazarotene • Macrolactams (calcineurin inhibitors): Tacrolimus & Pimecrolimus.
Response to topical therapy • Effects of topical therapy evident in 2-3 weeks • Clearing of scale is usually observed first, followed by flattening of the treated plaques • Resolution of erythema may take 6-8 weeks
Phototherapy 1. Extensive and widespread disease 2. Resistance to topical therapy
PUVA photochemotherapy (PUVA) • Combined use of a photosensitizing drug methoxsalen (8-methoxypsoralens) with UVA irradiation (320-400 nm) • Mechanism of action: 1. Interferes with DNA synthesis → decrease cellular proliferation 2. Induces apoptosis of cutaneous lymphocytes (localized immunosuppression).
Method of administering PUVA • 0.6mg/kg of 8-MOP(methoxypsoralen) given 2 hrs before irradiation • Initial dose of UVA is 2-5 J/cm2 with exposure time of 5 mins • PUVA administered 2-3 times per week in an outpatient setting. • Every week UVA dose increased by 20% and exposure time by 5 mins • Maintenance treatments every 2-4 weeks until remission • Relief with 20-30 treatments
Side Effects • Nausea, pruritus, burning sensation. • Long-term complications • photo damage to the skin • skin cancer
UVB phototherapy • Irradiation with light of wavelength 290-320 nm • Effective for moderate to severe psoriasis • Usually combined with one or more topical treatments like tar or anthralin • Narrow-band UVB phototherapy • Use of a fluorescent bulb with a narrow emission spectrum that peaks at 311 nm (UVB spectrum, 290-320 nm). • More effective than broadband UVB for the treatment of plaque-type psoriasis
Systemic Agents Indications: • Resistant to both topical treatment and phototherapy • Active psoriatic arthritis. • Physically, psychologically, socially or economically disabling disease • Steroids: only used in life threatening situations like erythrodermic & pustular psoriasis. • Cyclosporin: Immune modulator • Used in erythrodermic & resistant psoriasis • Limitations: expensive & nephrotoxic and hypertensive
Systemic Agents • Methotrexate: • Three doses of 2.5-5 mg orally 12 hrly or 7.5-15 mg single dose; administered every week. • Contraindicated in hepatic & renal diseases. Close monitoring of blood counts & hepatic function essential. • Acitretin: • For widespread psoriasis; combination with PUVA reduces total cumulative dose of UV irradiation • Contraindicated in pregnancy & women of child bearing age
Biological therapies Selective, immunologically directed intervention at key steps in the pathogenesis of the disease. Mechanism of action: • Inhibits the initial cytokine release and Langerhans cell migration • Targets activated T cells, prevents further T-cell activation, and eliminates pathologic T cells; • Inhibits proinflammatory cytokines, such as TNF
Biological therapies Indications: • Severe, recalcitrant cases • Psoriatic arthritis Mode of administration: • Intravenous, Subcutaneous Biological agents: • Efalizumab (Raptiva) • Etanercept (Enbrel ) • Infliximab (Remicade)
Prognosis • Course of plaque psoriasis is unpredictable. • Characterised by remissions and relapses • Often intractable to treatment • Relapses in most patients • Improves in warm weather • Poor Prognostic factors: Early onset, Family history, Stress, HIV infection