Download

1 / 33
1.3k likes | 3.86k Views
Shoulder Impingement Syndrome. Shoulder complex What is SIS What leads to worsening of SIS Causes of SIS Symptoms of SIS Hx Dx Physical examination Treatment Rehabilitation Manual Physical therapy techniques Stretching exercises

E N D
Shoulder complex • What is SIS • What leads to worsening of SIS • Causes of SIS • Symptoms of SIS • Hx • Dx • Physical examination • Treatment • Rehabilitation • Manual Physical therapy techniques • Stretching exercises • Preparation for strengthening exercises • Strengthening exercises • Physical therapist’s approaches toward SIS • PT products used in the treatment of SIS • Home exercise program Contents
Usually, there is enough room between the acromion and the rotator cuff so that the tendons slide easily underneath the acromion as the arm is raised. But each time you raise your arm, there is a bit of rubbing or pinching on the tendons and the bursa. With overuse, this can cause irritation and swelling of the bursa. What is shoulder impingement syndrome ?
Bone spurs : commonly caused by wear and tear of the acromioclavicularjoint. • In some people, the space is too small because the acromion is oddly sized. • So the acromion tilts too far down, reducing the space between it and the rotator cuff. If any other condition decreases the amount of space between the acromion and the rotator cuff tendons ! Impingement may get worse
Causes • joint stiffness (particularly the shoulder, neck or upper back) • shoulder instability • bony anomalies of the acromion or AC joint • muscle tightness (particularly the rotator cuff, pectorals and deltoid) • poor posture • inappropriate or excessive training • inadequate warm up • muscle weakness (especially the rotator cuff and scapula stabilisers) • muscle imbalances • inadequate rehabilitation following a previous shoulder injury or surgery • inappropriate technique (e.g. swimming stroke, tennis serve, throwing technique)
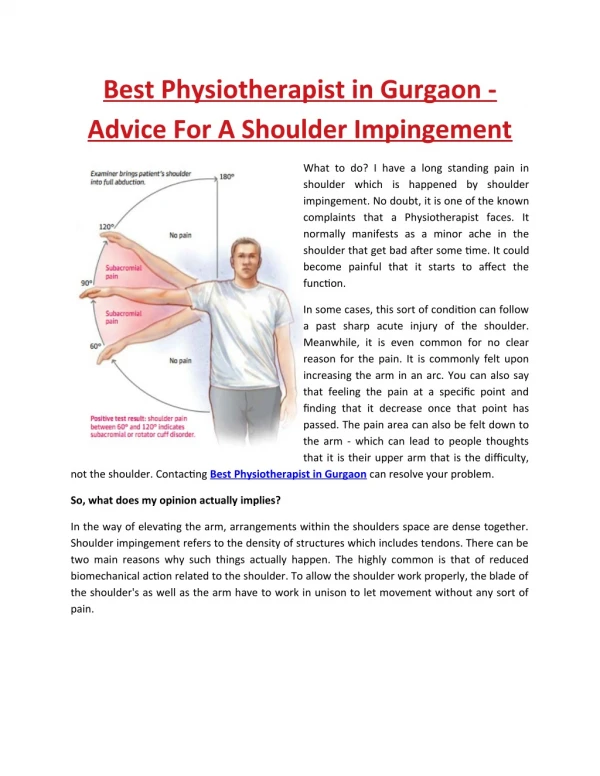
1-Pain: Exacerbated by over head or above the shoulder activities.Night pain often disturbing the sleep,particularly when the patient lies on the affected side. Onset of symptoms may be acute, following an injury or insidious. Particularly in older patients where no specific injury. In the acute stage1 there is painful arch abducton between 60 and 120˚ increased with resistance at 90˚. 2-Loss of motion: Prolonged shoulder pain causes the patient to restrict instinctively the range of use and often results in an initial adhesive capsulitis. 3-Weakness and inability to raise the arm: Indicates that the rotator cuff tendons are actually torn. Hx
medical history and physical examination- detailed questions about your activities and your job X-rays magnetic resonance imaging (MRI) scan- shows fluid inflammation in the bursa and the rotator cuff & tear of the tendons An arthrogram- helpful to detect rotator cuff tear. DiagnosisWhat tests will my doctor run?
In some cases, it is unclear whether the pain is coming from the shoulder or a pinched nerve in the neck. An injection of a local anesthetic (such as lidocaine) into the bursa can confirm that the pain is in fact coming from the shoulder. If the pain goes away immediately after the injection, then the bursa is the most likely source of the pain. Pain from a pinched nerve in the neck would almost certainly not go away after an injection into the shoulder.
Physical examinations 1.Manual motor testing for the rotator cuff muscles: Geber’s lift-off test for subscapu;aris- Get the patient in standing position. He is asked to place hand behind the back with dorsum of his hand resting in the mid lumbar spine region. Ask to raise the hand off the back increasing internal rotation of the humerus and extention at the shoulder Positive: inability to move the dorsum of the hand off the back constitutes an abnormal lift-off test and indicates subscapularis rupture or dysfunction
2.The key feature of the physical examination: assessment for the signs of impingementa-Neer impingement sign: with patient sitting or standing the place one hand on the posterior aspect of the scapula to stabilize the shoulder girdle, and with the other hand take the patient’s internally rotated arm by the wrist and place it In full forward flexion.If there is impingement the patient will complain of a pain in the range of 70˚-120˚of forward flexion as the rotator cuff comes into contact with the rigid coracoacromial arch.
b –Hawkin’s impingement sign: with the patient sitting or standing the examiner places the patient’s arm in 90˚ of forward flexion and forcefully internally rotates the arm, bringing the greater tuberosity in contact with the lateral acromion. A (+)Ve result is indicated if pain is reproduced during the forced internal rotation at the supraspinatus site.
Maintain the strength in the muscles of the rotator cuff. • These muscles help control the stability of the shoulder joint. Strengthening these muscles can actually decrease the impingement • Therapist can also evaluate your workstation or the way you use your body when you do your activities and suggest changes to avoid further problems Rehabilitation
Recommended early in the recovery period. • to help maintain joint mobility and flexibility of the muscles and tendons in the shoulder. • should not feel more than mild pain with any range-of-motion/flexibility exercise • sharp or tearing pain while stretching, stop exercising immediately SHOULDER IMPINGEMENT SYNDROME STRETCHING EXERCISES
The joint should always be heated for five minutes and stretched with range-of-motion exercises before beginning strengthening exercises Preparing for strengthening exercises
Weighted pendulum stretch weighted pendulum stretching exercise performs two functions:1.Gently stretches the space in which the tendons pass to relieve pressure on the tendons2.Prevents the development of a frozen (stiff) shoulderThis exercise can be started almost immediately after a shoulder injury, or after receiving a steroid injection into the shoulder joint. This exercise should be performed after heating for five minutes once or twice per day.
Relax your shoulder muscles While standing or sitting, keep your arm vertical and close to your body (bending over too far may pinch the rotator cuff tendons) Allow your arm to swing forward to back, then side to side, then in small circles in each direction (no greater than 1 foot in any direction). Only minimal pain should be felt. Stretch the arm only (without added weight) for three to seven days. Progress this exercise by adding 1 to 2 pounds (0.5 to 1 kg) each week and gradually increasing the diameter of the movements (not to exceed 18 to 24 inches or 45 to 60 cm ) After a few weeks this exercise should be supplemented or replaced by other exercises to target specific areas of tightness/restriction. The pendulum stretch may be recommended as a warm up for more localized flexibility exercises and/or strengthening exercises.
necessary to improve shoulder muscle strength and help to prevent further injury. These exercises can often be started approximately one to two weeks after beginning the pendulum stretch exercises, once any acute inflammation has resolved, or after having a steroid injection into the shoulder joint. Muscle-strengthening exercises
PartA:hold the elbow at 90°, close to the side. The rubber band is hooked onto a door handle and grasped with the hand. The forearm is slowly moved towards the body 2 to 3 inches, and held for 5 seconds. The hand should not rotate as the forearm moves. Part B: The outward rotation isometric exercise is performed with the elbows at 90°, close to the sides. The rubber band is grasped with the hands. The formearms are moved outward 2 to 3 inches and held for 5 seconds. Sets of 15 to 20 exercises, each held for 5 seconds, should be performed daily. Strengthening exercises for the rotator cuff tendons
Lie on the back with your knees bent and feet flat. arms should be straight out,15 to 30 cm away from the side of the body, with palms facing upward. Keeping the low back flat against the ground, squeeze your shoulder blades downward and towards each other, towards the spine. Do not shrug the shoulders and keep the neck relaxed. Doer should feel the lower muscles between the shoulder blades contracting. Hold for five seconds and repeat 20 times. Do this exercise two to three times per day. Scapular squeezes
Hold your elbows at 90 degrees, close to your sides; holding a towel between your torso and the inside of your elbow will cue you to keep your elbow by your side. • Hold one end of a rubber band in each hand and rotate the affected forearm outward two or three inches • Holding for five seconds Outward rotation exercise
Ensure an optimal outcome and reduce the likelihood of recurrence in all patients with shoulder impingement. • soft tissue massage • electrotherapy (e.g. ultrasound, TENS etc) • stretches • joint mobilization • joint manipulation • ice or heat treatment • exercises to improve strength, flexibility, posture and scapula stability • correction of abnormal biomechanics or technique • education • postural taping • the use of a posture support • anti-inflammatory advice • activity modification advice • a gradual return to activity program Physiotherapy for shoulder impingement
Physiotherapy products for shoulder impingement Some of the most commonly recommended products by physiotherapists to hasten healing and speed recovery in patients with shoulder impingement include: Slings Shoulder Supports Ice Packs Sports Tape (for postural taping) Posture Supports Resistance Band (for strengthening exercises) TENS Machines (for pain relief) Therapeutic Pillows