Download
1 / 4
40 likes | 346 Views
PROBLEM: Subacromial Impingement Syndrome. PIER Document Series on Evidence-based Practice in Physical Therapy. What is subacromial impingement syndrome (SIS)?

E N D
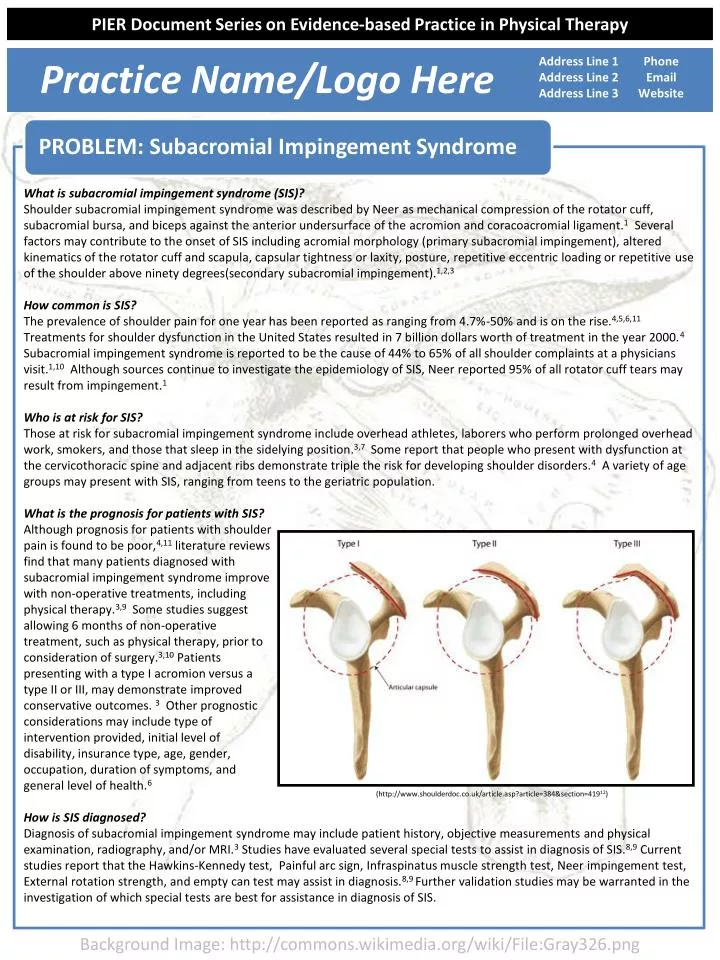
PROBLEM: Subacromial Impingement Syndrome PIER Document Series on Evidence-based Practice in Physical Therapy What is subacromial impingement syndrome (SIS)? Shoulder subacromial impingement syndrome was described by Neer as mechanical compression of the rotator cuff, subacromial bursa, and biceps against the anterior undersurface of the acromion and coracoacromial ligament.1 Several factors may contribute to the onset of SIS including acromial morphology (primary subacromial impingement), altered kinematics of the rotator cuff and scapula, capsular tightness or laxity, posture, repetitive eccentric loading or repetitive use of the shoulder above ninety degrees(secondary subacromial impingement).1,2,3 How common is SIS? The prevalence of shoulder pain for one year has been reported as ranging from 4.7%-50% and is on the rise.4,5,6,11 Treatments for shoulder dysfunction in the United States resulted in 7 billion dollars worth of treatment in the year 2000.4Subacromial impingement syndrome is reported to be the cause of 44% to 65% of all shoulder complaints at a physicians visit.1,10 Although sources continue to investigate the epidemiology of SIS, Neer reported 95% of all rotator cuff tears may result from impingement.1 Who is at risk for SIS? Those at risk for subacromial impingement syndrome include overhead athletes, laborers who perform prolonged overhead work, smokers, and those that sleep in the sidelying position.3,7 Some report that people who present with dysfunction at the cervicothoracic spine and adjacent ribs demonstrate triple the risk for developing shoulder disorders.4 A variety of age groups may present with SIS, ranging from teens to the geriatric population. What is the prognosis for patients with SIS? Although prognosis for patients with shoulder pain is found to be poor,4,11 literature reviews find that many patients diagnosed with subacromial impingement syndrome improve with non-operative treatments, including physical therapy.3,9 Some studies suggest allowing 6 months of non-operative treatment, such as physical therapy, prior to consideration of surgery.3,10 Patients presenting with a type I acromion versus a type II or III, may demonstrate improved conservative outcomes. 3 Other prognostic considerations may include type of intervention provided, initial level of disability, insurance type, age, gender, occupation, duration of symptoms, and general level of health.6 How is SIS diagnosed? Diagnosis of subacromial impingement syndrome may include patient history, objective measurements and physical examination, radiography, and/or MRI.3 Studies have evaluated several special tests to assist in diagnosis of SIS.8,9 Current studies report that the Hawkins-Kennedy test, Painful arc sign, Infraspinatus muscle strength test, Neer impingement test, External rotation strength, and empty can test may assist in diagnosis.8,9 Further validation studies may be warranted in the investigation of which special tests are best for assistance in diagnosis of SIS. Practice Name/Logo Here Address Line 1 Address Line 2 Address Line 3 Phone Email Website • (http://www.shoulderdoc.co.uk/article.asp?article=384§ion=41912) Background Image: http://commons.wikimedia.org/wiki/File:Gray326.png
EVIDENCE • INTERVENTION PIER Document Series on Evidence-based Practice in Physical Therapy What evidence exists to support the use of manual therapy techniques in patients with SIS? Evidence suggests that both long term and short term gains in pain and functional use of the shoulder are noted in patients receiving manual therapy techniques aimed at the cervicothoracic spine and ribs.4,13-17 Bergman et al13 compared standard primary care in patients with shoulder pain to a group receiving manual therapy interventions plus primary care. The group receiving the additional manual therapy demonstrated statistically significant improvements at 26 and 52 weeks. At one year, the standard care group had only made gains similar to those produced by the manual therapy group at just 12 weeks. Strunce et al14 looked at short term effects of manual therapy interventions in patients with a primary complaint of shoulder pain. Following just one treatment, statistical improvements in shoulder ROM and pain were made in 20 out of 21 subjects after interventions to the cervicothoracic spine and ribs. No direct treatment to the shoulder was performed. Conversely, direct shoulder mobilizations in the absence of treatment to the cervicothoracic spine have not been shown to produce statistically significant improvements.18 Is there any evidence to support the use of exercise in patients with SIS? Posture correction exercises that consider upper quadrant posture of the humerus and scapula in combination with cervical and thoracic spine posture have been encouraged in patients with SIS.19,20,21 Promoting cervical retraction and erect posture may promote increases in the subacromial space as measured by the acromiohumeral distance.21,22,23 Flexibility exercises to stretch the muscles of the anterior and posterior shoulder girdle muscles have been recommended based upon the conclusions of a systematic review of twelve randomized clinical trials evaluating the effectiveness of exercise in treating patients with SIS.9 Stretching focused upon the posterior capsule of the shoulder joint and the joints of the thoracic spine may also be beneficial for these patients.19,20 Exercises to promote neuromuscular re-education are advocated to balance the function of the muscles of throughout the shoulder girdle including the scapula. 22 In particular, exercises promoting lower trapezius, middle trapezius, and serratus anterior activation with minimal activity in the upper trapezius are recommended.20,22 • What interventions do physical therapists utilize in treating patients with diagnosed with SIS? • Manual Therapy Techniques • Therapeutic Exercise • Posture, Movement, and Ergonomic Training • Taping Techniques • Electrophysical Agents • (Mintken et al4) • (Tate et al20) Background Image: http://commons.wikimedia.org/wiki/File:Gray326.png
EVIDENCE • REFER PIER Document Series on Evidence-based Practice in Physical Therapy Is there any evidence to support the use of exercise in patients with SIS? (Continued) Once efficient motor control is established, strengthening exercises are recommended. Targeted strengthening of the rotator cuff and scapular muscles has been associated with positive treatment outcomes in patients with SIS.9,16,19,20,23,24 Additionally, there is some evidence that indicates emphasizing performance of these exercises below 90 degrees of shoulder elevation may be superior to performing them above 90 degrees.24 Functional integration involves the implementation of a whole-body kinetic-chain approach to strengthening multiple joints simultaneously and during movement patterns that mimic athletic and functional daily activities of living.21 Such exercises have been utilized as a component of an approach associated with positive outcomes in patients receiving physical therapy intervention for SIS.20 Is there evidence to support the use of other treatments offered by physical therapists form patients with SIS? Ergonomic interventions including the use of an arm support and an alternative mouse have been shown to decrease the incidence of musculoskeletal shoulder disorders.25 Postural interventions involving changes made in one or more of the components of posture may have a positive effect on shoulder range of movement and the range at which pain is experienced.26 Various forms of taping may be beneficial for patients with SIS. Kinesio taping may be of some usefulness for increasing pain free active ROM immediately after application27 and has also been found to be more effective than local modalities during the first two weeks of treatment.28 Scapular taping has been shown to decrease upper trapezius and increase lower trapezius muscle recruitment during shoulder elevation.29 Participants with SIS receiving high intensity laser therapy had greater improvements in pain and ROM than participants receiving ultrasound.30 With no significant differences observed at a 1-year follow-up, patients with SIS were found to benefit equally from supervised exercise and radial extracorporeal shockwave therapy.31 We strive to provide care based on the best current evidence available for guiding physical therapy practice. For your patients with SIS, our approach will emphasize a combination of manual physical therapy techniques applied throughout the upper quarter, therapeutic exercise emphasizing functional progression, and patient education in postural and ergonomic modifications. Adjunctive treatments such as taping or electrophysical agents that have demonstrated utility in aiding the management of SIS may also be used as indicated and necessary. • (Tate et al20) • (Tate et al20) • (Tate et al20) Background Image: http://commons.wikimedia.org/wiki/File:Gray326.png
REFERENCES PIER Document Series on Evidence-based Practice in Physical Therapy • Mcclure PW, Michener LA, Karduna AR. Shoulder Function and 3-Dimensional Scapular Kinematics in People With and Without Shoulder Impingement Syndrome. Phys Ther. 2006; 86(8): 1075-1090. • Schmitt L, Snyder-Mackler L. Role of Scapular Stabilizers in Etiology and Treatment of Impingement Syndrome. J Orthop Sports Phys Ther. 1999;29(1):31-38. • Bigliani LU, Levine WN. Current Concepts Review Subacromial Impingement Syndrome. J Bone Joint Surg. 1997;79-A(12):1854-1868. • Mintken PE, Cleland JA, Carpenter KJ, Bieniek ML, Keirns M, Whitman JM. Some factors predict successful short-term outcomes in individuals with shoulder pain receiving cervicothoracic manipulation: a single-arm trial. Phys Ther. 2010 Jan;90(1):26-42. • Vind M, Bogh SB, Larsen CM, Knudesen HK, Sogaard K, Juul-Kristensen B. Inter-examiner reproducibility of clinical tests and criteria used to identify subacromial impingement syndrome. BMJ Open. 2011;1(1). • Kennedy CA, Manno M, et al. Prognosis in Soft Tissue Disorders of the Shoulder: Predicting Both Change in Disability and level of Disability After Treatment. Phys Ther. 2006; 86: 1013-1032. • Tangtrakulwanich B, Kapkird A. Analyses of possible risk factors for subacromial impingement syndrome. World J Orthop. 2012 Jan 18;3(1):5-9. • Michener LA, Walsworth MK, Doukas WC, Murphy KP. Reliability and diagnostic accuracy of 5 physical examination tests and combination of tests for subacromial impingement. Arch Phys Med Rehabil. 2009 Nov;90(11):1898-903. • Michener LA, Walsworth MK, Burnet EN. Effectiveness of Rehabilitation for Patients with Subacromial Impingement Syndrome. J Hand Ther. 2004;17:152-164. • Park HB, Yokota A, Gill HS, El Rassi G, McFarland EG. Diagnostic accuracy of clinical tests for the different degrees of subacromial impingement syndrome. J Bone Joint Surg Am. 2005 Jul;87(7):1446-55. • Kuijpers T, A.W.M. Van derWindt, D, Joan A, Boeke, P, Twisk JWR, Vergouwe Y, Bouter LM, J.M.G. Van derHeijden G. Clinical prediction rules for the prognosis of shoulder pain in general practice. Pain. 2006;120:276-285. • Shoulderdoc.co.uk. Rotator Cuff Biomechanics. Available at: http://www.shoulderdoc.co.uk/article.asp?article=384§ion=419.Accessed September 27, 2012. • Bergman GJ, Winters JC, Groenier KH, Pool JJ, Meyboom-de Jong B, Postema K, van derHeijden GJ. Manipulative therapy in addition to usual medical care for patients with shoulder dysfunction and pain: a randomized, controlled trial. Ann Intern Med. 2004 Sep 21;141(6):432-9. • Strunce JB, Walker MJ, Boyles RE, Young BA. The immediate effects of thoracic spine and rib manipulation on subjects with primary complaints of shoulder pain. J Man ManipTher. 2009;17(4):230-6. • Boyles RE, Ritland BM, Miracle BM, Barclay DM, Faul MS, Moore JH, Koppenhaver SL, Wainner RS. The short-term effects of thoracic spine thrust manipulation on patients with shoulder impingement syndrome. Man Ther. 2009 Aug;14(4):375-80. • Bang MD, Deyle GD. Comparison of supervised exercise with and without manual physical therapy for patients with shoulder impingement syndrome. J Orthop Sports Phys Ther. 2000 Mar;30(3):126-37. • McClatchie L, Laprade J, Martin S, Jaglal SB, Richardson D, Agur A. Mobilizations of the asymptomatic cervical spine can reduce signs of shoulder dysfunction in adults. Man Ther. 2009 Aug;14(4):369-74. • Yiasemides R, Halaki M, Cathers I, Ginn KA. Does passive mobilization of shoulder region joints provide additional benefit over advice and exercise alone for people who have shoulder pain and minimal movement restriction? A randomized controlled trial. Phys Ther. 2011 Feb;91(2):178-89. • Holmgren T, Hallgren H, Oberg B, Adolfsson L, Johansson K. Effect of specific exercise strategy on need for surgery in patients with subacromial impingement syndrome: randomised controlled study. BMJ. 2012; 344 e787. • Tate A, McClure P, Young I, Salvator R, Michener L. Comprehensive impairment-based exercise and manual therapy intervention for patients with subacromial impingement syndrome: a case series. J Orthop Sports Phys Ther. 2010; 40(8):474-493. • Reinold M, Escamilla R, Wilk K. Current concepts in the scientific and clinical rationale behind exercises for glenohumeral and scapulothoracic musculature. J Orthop Sports Phys Ther. 2009; 39(2):105-117. • Kalra N, Seitz A, Boardman N, Michener L. Effect of posture on acromiohumeral distance with arm elevation in subjects with and without rotator cuff disease using ultrasonography. J Orthop Sports Phys Ther. 2010;40(10):633-640. • Cools A, Dewitte V, Lansxweert F, Notebaert D, Roets A, Soetens B, Cagnie B, Witvrouw E. Rehabilitation of scapular muscle balance: which exercises to prescribe? Am J Sports Med. 2007; 35; 1744-1752. • Celik D, Akyuz G, Yeldan I. Comparison of the effects of two different exercise programs on pain in subacromial impingement syndrome. ActaOrthopTraumatolTurc. 2009;43(6):504-509. • Hoe VCW, Urquhart DM, Kelsall HL, SIM MR. Ergonomic design and training for preventing work-related musculoskeletal disorders of the upper limb and neck in adults (Review). The Cochrane Collaboration. 2012; 8. • Lewis JS, Wright C, Green A. Subacromial impingement syndrome: The effect of changing posture on shoulder range of movement. J Orthop Sports Phys Ther. 2005;35(2):72-87. • Thelen MD, Dauber JA, Stoneman PD. The clinical efficacy of kinesio tape for shoulder pain: A randomized, double-blinded, clinical trial. J Orthop Sports Phys Ther. 2008;38(7):389-395. • Kaya E, Zinnuroglu M, Tugcu I. Kinesio taping compared to physical therapy modalities for the treatment of shoulder impingement syndrome. ClinRheumatol. 2011;30(2):201-207. • Selkowitz DM, Chaney C, Stuckey SJ, Vlad G. The effects of scapular taping on the surface electromyographic signal amplitude of shoulder girdle muscles during upper extremity elevation in individuals with suspected shoulder impingement syndrome. J Orthop Sports Phys Ther. 2007;37(11):694-702. • Santamato A, Solfrizzi V, Panza F, et al. Short-term effects of high-intensity laser therapy versus ultrasound therapy in the treatment of people with subacromial impingement syndrome: A randomized clinical trial. Phys Ther. 2009;89(7):643-652. • Engebretsen K, Grotle M, Bautz-Holter E, Ekeberg OM, Juel NG, Brox JI. Supervised exercises compared with radial extracorporeal shock-wave therapy for subacromial shoulder pain: 1-year results of a single-blind randomized controlled trial. Phys Ther. 2011;91(1):37-47. Background Image: http://commons.wikimedia.org/wiki/File:Gray326.png