Download
1 / 37
370 likes | 396 Views
Learn about the stepped approach to managing atopic eczema using emollients, additives, bathing, moisturizers, and other treatments. Understand the importance of proper education, potency, age considerations, and side effects.

E N D
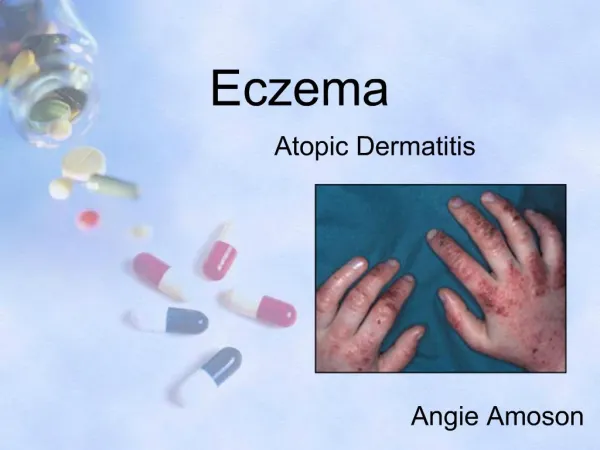
Topical Therapies for Eczema Sandra Lawton Nurse Consultant Dermatology sandra.lawton@nuh.nhs.uk
Treatment: stepped approach to management • Use a stepped approach for managing atopic eczema: • tailor treatment step to severity • use emollients all the time • step treatment up or down as necessary • Provide: • information on how to recognise flares • instructions and treatments for managing flares
Case Study • Age 5 • School • Statement • Sleep Terrible • Repeat Prescriptions+++++ • Chaotic routine • Admission
EmollientsWhich one is best??? • Soap Substitutes • Bath Oils • Shower • Moisturisers • Others
Soothe Soften Hydrate Protect Anti-inflammatory Anti-pruritic Steroid-sparing effect Effects of Emollients
Additives • Emollients may have ingredients added : • preservatives such as chlorocresol and parabens) • antiseptics such as benzalkonium chloride, • antipruritics such as lauromacrogols). • These added ingredients can act as irritants or allergens and provoke sensitisation or an immune response.
Humectants • Humectants are substances introduced into the stratum corneum to increase its water-holding capacity. The mode of action involves the active movement of water from the dermis to the epidermis. • Humectants include propylene glycol, lactic acid, urea and glycerol. • Some creams and lotions contain a mixture of occlusive and humectant substances – the humectant draws water into the epidermis, while the occlusive element ensures that it is trapped there.
Bathing • Bathing is useful for cleansing the skin, removing scale and previous topical therapies. • Bathing will also hydrate the skin and this is an ideal time to apply an emollient providing a lipid film, which prevents water evaporation from the epidermis.
Bath oils should disperse if added to bath water – not be an oil slick • Follow instructions re quantity added to bath water • Irritant effect – did not follow instructions regarding how many capfuls of Oilatum Plus Bath Oil
Patients Age Patients Lifestyle Previous Topical Therapy Availability Demonstrate Parent / patient choice Appropriateness Cost Adequate Supplies Considerations when prescribing emollients
Other Issues for patients • Does it smell? • Texture and consistency – how easy it is to apply? • Does it make the skin too shiny? • Does it make clothes greasy? • Packaging – tubes and pumps are popular. • Can it be used as a soap substitute? • Is it so greasy that it spoils school work? • Does it sting?
Treatment: emollients • Emollients should be: • unperfumed • used every day • prescribed in large quantities (250–500 g/week) • easily available to use at nursery, pre-school or school.
Treatment: topical corticosteroids • Potency should be tailored to severity: • mild potency for face and neck, except for 3–5 days of moderate potency for severe flares • moderate or potent preparations for short periods only for flares in vulnerable sites • do not use very potent preparations in children without specialist dermatological advice
Amount : Finger tip method v tube size Frequency : 1v 2 x daily. Vehicle Bursts Age Disease severity Surface area Site Occlusion Other treatments Patient preference Application
Local side-effects • spread and worsening of untreated infection; • thinning of the skin • irreversible striae and telangiectasia; • contact dermatitis; • perioral dermatitis • acne at the site of application in some patients
Tachyphylaxis • “Loss of effect” • Depends upon: • Usage frequency • Potency • Is reversible • Recommend change of topical steroids
Topical Calcineurin Inhibitors • Second line treatment for atopic eczema • Pimecrolimus cream (Elidel) • Tacrolimus 0.03% or 0.1% ointment (Protopic) • Effective, and increasingly used • Used to prevent flares • Initiated by physician with interest in dermatology • Unknown long term risk of skin cancer
Bandaging and suits To improve emollient effect Wet/dry garments Young infants with very dry skin To cover areas to stop scratching Impregnated bandages eg ichthopaste/steripaste Older children with limb or finger eczema
Education and adherence to therapy • Spend time educating children and their parents or carers about atopic eczema and its treatment. • Provide written and verbal information with practical demonstrations about: • how much of the treatments to use • how often to apply treatments • when and how to step treatment up or down • how to treat infected atopic eczema.
NICE Guideline • Atopic eczema in children • Management of atopic eczema in children from birth up to the age of 12 years • www.nice.org.uk/CG057