Download
1 / 38
380 likes | 523 Views
in + care Campaign Meet the Author July 11, 2012. Ground Rules for Webinar Participation. Actively participate and write your questions into the chat area during the presentation(s) Do not put us on hold Mute your line if you are not speaking (press *6, to unmute your line press #6)

E N D
in+care CampaignMeet the Author July 11, 2012
Ground Rules for Webinar Participation Actively participate and write your questions into the chat area during the presentation(s) Do not put us on hold Mute your line if you are not speaking (press *6, to unmute your line press #6) Slides and other resources are available on our website at incareCampaign.org All webinars are being recorded
Agenda • Welcome & Introductions, 5min • Meet the Author – Dr. Nikki Cockern, 30min • Q & A Session, 20min • Updates & Reminders, 5min
Retention of HIV+ Youth in Care:Lessons Learned & New Directions Nikki Cockern, PhD Horizons Project Wayne State University School of Medicine July 11, 2012 **Funded by HRSA, MDCH, and United Way**
Defining Retention • Retention • Keeping or holding of something: the act of retaining something or the condition of being retained • Memory: the ability to remember things • The continued possession, use or control of something
What Constitutes Retention? • Follow-up appointments at least every 3-6 months • Routine monitoring of CD4 counts and viral loads • ART treatment and adherence counseling • Primary care services • Prevention for positives
Retention Strategies • “One-stop shopping” & multidisciplinary approach to HIV care, that’s youth sensitive • Peer Advocacy • Transportation • Treatment Adherence Program • Lost to Follow-Up (L2FU) Program
Kids were still missing appointments! What else could we do? Our outreach & prevention teams obtained research dollars to implement & assess outreach & behavioral interventions to improve testing and care Results from their SPNS initiatives had a direct impact on clinical services Interventions in other medical clinics that were multi-systemic in nature were also proving to be effective in positive behavior change
Shift How We Do Business Starts with a paradigm shift Examine how we (providers) think about the teens we serve What type of language do we use (assets vs. risk) Move from (implied) superiority Develop cultural competence Empowerment: Give youth an opportunity to be the “expert”; demonstrate mutual respect & partnership Address stigma, assumptions, judgmental behavior within the care delivery system Provide integrated peer driven medical and psychological support models Address the ‘real affects’ of denial and depression while increasing hopefulness and opportunities for success
Using what we know to foster supportive teen interactions THEORETICAL MODELS
Factors Associated with Change • Cognitive Processes • Self-Efficacy – Confidence and Temptation • Decisional Balance (importance & skill) • Interference with Readiness to Change • Drug Use • Emotional Distress • Lack of Social Support • Family/Marital/Partner Conflict
Motivational Interviewing (MI) • Evidenced based intervention to promote health behavior change • MI is • client-centered, • goal-oriented approach • focused on increasing intrinsic motivation for change by: • resolving ambivalence about different potential courses of action • and increasing self-efficacy about change *Miller & Rollnick (2002, 2007)
What does this look like in a conversation? Empathic and warm Listening and understanding Expressing optimism and hope Reinforcing specific strengths Emphasizing personal choice and responsibility Offering menu of options Discussing value-behavior incongruence
Why MI? • Client-centered and youth friendly • Appropriate for those in earlier stages of behavior change • Validated with substance use, condom use, and health behaviors • at-risk youth and youth living with HIV
Advantages of MI • Client-centered intervention • Can be performed by a variety of staff members • Occurs in a natural setting • Ambivalence is addressed
Horizons’Interventions Using MI • Brothers Saving Brothers (BSB) • MI for HIV Outreach to Encourage HIV testing among young African American men who have sex with men • MI for Youth Engagement in HIV Care • MI for Medication Adherence and Secondary Prevention • Computer applications – Motivational Enhancement System for adherence and sexual risk (adapted from Ondersma et al.)
Brothers Saving Brothers (BSB) Three session group level prevention intervention for YAAMSM delivered to youth residing in DMA that addresses: Ethnic and gay identity Partner negotiation Sexual risk reduction HIV risk and vulnerability N=37 (16-24 years of age; mean age=18) 100% completed 1 session 89% completed 2 sessions 86% completed 3 sessions 98% reported high satisfaction with intervention & staff 17
Brothers Saving Brothers (BSB), Cont • MI during outreach to encourage HIV C&T • Single session (30 minutes) as part of field outreach for HIV C&T (to get tested and return for results (OraSure testing)) (N=188 ages 16-24 (Mean=19.79) • Random assignment to Outreach plus MI (N=96) or Traditional Outreach (N=92) • Baseline survey inquired about risk behaviors and readiness to change risk behaviors • Peer staff (high school degree or equivalent) • Findings: More youth in MI condition tested immediately after the session (49% vs. 20%) & returned for test results @ significantly higher rate than Outreach alone condition (98% vs. 72%)
MI for Engagement in Care • Single session (30 minutes) delivered at baseline and 6 months focusing on engagement and retention in care • Randomized to Masters prepared staff vs. Peer staff (high school degree or equivalent) • Findings: Both groups improved regularity of primary care appointments • Effect size for peer staff was larger than Masters prepared staff
MI for Medication Adherence & Secondary Prevention • 4 sessions (60 minutes) delivered over 6 weeks focusing on 2 of 3 behaviors (i.e., substance use, unprotected sex, and medication adherence) • Randomized to intervention (psychology graduate students) vs. wait-list control • Findings: Intervention group significantly greater reduction in unprotected sex acts and viral load at 3 month follow-up
MI Computer Applications • Motivational Enhancement System for sexual risk (adapted from Ondersma et al.) & adherence • MISTI (Sexual Risk)(Feasibility study) (N=26) • Youth randomized to a single session face-to-face (doctoral staff member) or computer delivered intervention • MISTI-II (Sexual Risk) (N=54) • Youth receive single session computer delivered intervention and 3 month follow-up (88% retention) • MESA (Adherence) • Youth randomized to a 2 session computer-delivered intervention
Motivational Enhancement System • Intervention programmed with CIAS using principles of Motivational Interviewing • Evocation – elicit responses from participant including desire, ability, reasons and need for change • Collaboration – participant chooses goal while interventionist (computer character) reflects choices, gives affirmations, offers information and advice when requested by participant • Autonomy – interventionist emphasizes personal choice, asks for permission to give information (participant can say no!); participant may choose to change behavior, not to change behavior, to think about change • Tailored based on MOTIVATION (Readiness)
MISTI Feasibility Results • 100% of patients in the computer condition (11/11) completed their intervention session • 69% of patients in the in-person condition (9/13) completed their intervention session • Patient Evaluations (items rated on scale of 1-4): • How helpful? M = 3.52 (SD = 0.75) • How honest? M = 3.90 (SD = 0.30) • Recommend Project MISTI? M = 3.52 (SD = 0.51)
MISTI Evaluation Results - % of Sample 12 months post baseline 3 month post test
To Sum Up…… • MI interventions were helpful in reducing sexual risk and substance use, and aided in increasing attendance • We decided to train our entire staff in MI to enhance the conversations we had with youth • Innovation is as essential to programming for youth as nonjudgmental staff
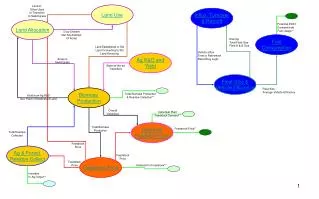
Improvement Process-Missed Appointment ProcessYouth who have missed a scheduled medical clinic appointment, without contacting team and scheduling another within 30 days. List Prioritization1. Clients who missed their clinic appointment within the first month (21-30) days and have not rescheduled2. Clients who have not attended a clinic appointment in 2-6 months3. Clients who have not attended a clinic appointment in 6-12 months 1. Maintain List Identify youth who missed clinic appt. & not able to reschedule 5. Contact made w/ Client & clinic visit scheduled Or Repeat 2. 1st month after missed clinic visit. Advocate attempts Contact via phone/text 4. 3rd month Home Visit 3. 2nd month Mail post Card sent MI @ point of contact & @ clinic appt. MI via phone MI @ HV if contact made
Other Projects • Interventions to increase medication adherence among children youth, and young adults • Healthy Choices • A+ (Adolescent and Young Adult Positive Living through Understanding and Support) • This is framed as “a program for young adults that want to make healthier choices as it relates to their medical care and maintenance of a safe viral load”.
Healthy Choices PLUS PathwayReferral Criteria: VL>1000 on one active drug or self-report <80% adherence with detectable viral load, ages 16-29 (will consider younger if no family for CHIP program) Failure Success Relapse Failure Success If youth drops out of treatment after less than ¾ of sessions completed, then return to beginning of planned intervention when they return
To retain Youth • We continue doing what has worked • Maintain Youth Tracking Log • Contact youth to • confirm before appointments, • if missed then during appointments or as soon as possible after missed appointment • Continue use of • Social media: texting and Facebook • Motivational Interviewing integrated into calls, home visits, and clinical appointments
The Use of MI in the Continuum of Care During HIV prevention & counseling sessions, especially around safe sex; reducing sexual risk; communicating w/partners On the phone w/clients who cancel or make excuses about missing medical appointments (during appointment reminder calls) With patients who are not adherent to medication During initial meeting (medical visit/intake) to encourage engagement in treatment, identify strengths Use MI to help youth realize their behavior doesn‘t match their value
Next Steps • Formally evaluate the effects of MI in clinic setting (with new youth, those returning after extended absence) • Effective/Useful with increasing clinic attendance following MI (short vs. long term effects) • Examine timing of intervention (is there an impact) • Venue of intervention (i.e. face-to-face, phone, text) • Provide youth who continue to have greater difficulty with more intensive interventions when feasible.
Staff Acknowledgement Director of Medical Service and Research: Elizabeth Secord, MD Director of Prevention Services:Angulique Outlaw, PhD Consultant for Psychological Services and Research: Sylvie Naar-King, PhD ATN Behavioral Research Coordinator: Monique Green Jones, MPH ATN Clinical Research Coordinator:Charnell Cromer, MSN Clinical Care Manager: Nikki Cockern, PhD Clinical Nurse Practitioner: Debbie Richmond, NP Clinical Social Worker: Tiffani Hollowell, CMSW Care Coordinator/Case Manager: Keshaum Houston, BS Health Systems Navigator: ToliaMouzon, BS Adolescent Consultant: Jessica Daniel, MPH MSM Prevention Coordinator: Jeremy Toney MSM Outreach Worker:Bre’ Campbell ATN C2P Coordinator: Emily Halden Brown, MPP ATN Research Assistant: Cindy Chidi, BS Fisher HRH Prevention Coordinator: Angela Williams, MPH Fisher Outreach Worker:Te’Neice Dobbins, BS
Thank you!—Questions/Comments? Nikki Cockern, PhD; 313.745.4892; scockern@med.wayne.edu Monique Green-Jones, MPH; 313.966.9763mojones@med.wayne.edu http://www.peds.med.wayne.edu/horizons
Partners in+care • Partners in+care Secret Facebook Group is live! • Share tips, stories and strategies • Join a community of PLWH and those who love them • Email michael@nationalqualitycenter.org for more details • Partners in+care website is live! • http://www.incarecampaign.net/index.cfm/77453 • Join our mailing list (a list-serv version of the FB Group)
Upcoming Events and Deadlines • Campaign Office Hours: Mondays & Wednesdays 4-5pm ET • Improvement Update Submission Deadline: July 16, 2012 • Data Collection Submission Deadline: August 1, 2012 • Next Campaign Webinar: Substance Abuse and RetentionTuesday, July 31, 2012 4pm ET
Campaign Headquarters:National Quality Center (NQC)90 Church Street, 13th floor New York, NY 10007Phone 212-417-4730 incare@NationalQualityCenter.orgincareCampaign.org youtube.com/incareCampaign