Download
1 / 11
110 likes | 246 Views
Teaching from Review of the Progress Note. Tayloe Loftus, MD SUNY Syracuse Updated 2010 by Heather Harrell, MD, FACP University of Florida, Gainesville. Why Read a Student’s Note?. “Scut” Teaching! Identify student learning needs “Case-based” teaching better than lecture

E N D
Teaching from Review of the Progress Note Tayloe Loftus, MD SUNY Syracuse Updated 2010 by Heather Harrell, MD, FACP University of Florida, Gainesville
Why Read a Student’s Note? • “Scut” Teaching! • Identify student learning needs • “Case-based” teaching better than lecture • Ensures accuracy of the medical record
What are some of your “pet peeves” with students’ progress notes? • Too long • Too detailed • Not detailed enough • Not accurate • Lack plans • On the chart too late
How have you set expectations with students? • Practical suggestions • Heading • How should they label their note? • “Date, time, stamp, sign” • Hospitalization context (e.g. day # of antibiotics) • Length • ≤ 1 page, telegraphic language (don’t need complete sentence) • Organization (SOAP) • Timing (when should it be on the chart/EMR) • Billing/compliance issues
Setting Expectations: Data Reporting • Subjective • Patient’s input on major problems (minor concerns don’t need to go in the note) • Objective • Vital signs are vital, don’t forget them • Report pertinent exam (problem focused, exam changes, findings that change management) • Clarify how you want meds listed and how often
Setting Expectations: Avoiding the “SOP” Note • Assessment/Plan- Diagnosis-based, not systems-based • Commit to a working diagnosis and plan for each problem before discussing the case with you • Prioritize problems/diagnoses • Brief assessments reflecting the most current thinking (not summaries of the whole hospitalization) • Plans should include therapeutic endpoints for discharge/care transition planning • Addenda • Clarify when should notes be addended
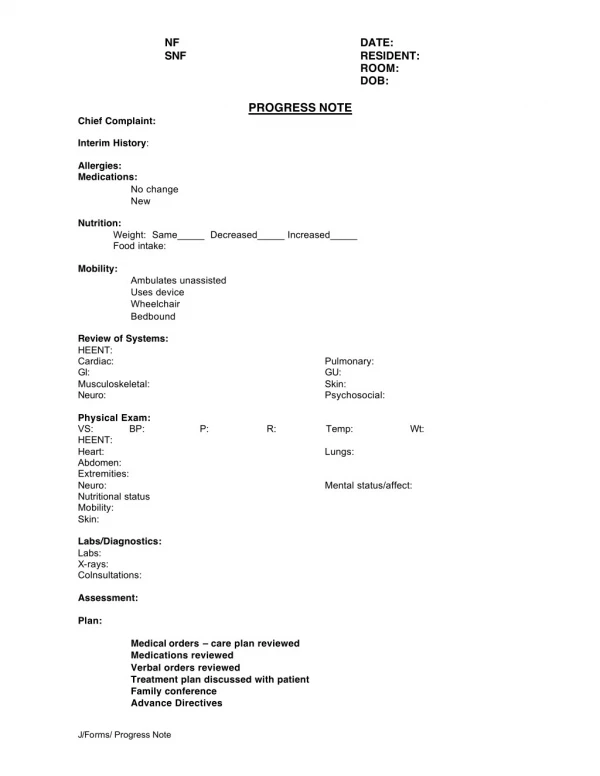
Sample Notes • What can you learn about the student from this note
What can you learn about a student from the note? • Communication skills • Organizational skills • Professionalism (timeliness, plagiarism) • Physical examination skills • Components – HEENT, lymph nodes, neuro • Meaning – “no tactile fremitus” • Knowledge physical manifestations of disease e.g. omitting JVD or S3 assessment in patient with CHF
What MORE can you learn about a student from the note? • Clinical reasoning • Pertinent +/-’s • Appropriate prioritization of problems • Accurate representation of team’s reasoning • “Icing on the Cake” (Manager-level behavior) • Interesting additions to care? • Evidence of reading? • Attention to “finer points” (PT/OT, d/c plans)
Giving Feedback on Notes • “Scut” Teaching! • Timing (end of day, interval options) • Multiple notes (read all/review one, cull comments) • Plan to address identified student issues • If no/little progress, “demo” note
Author Contact Information Tayloe Loftus, MD Loftust@upstate.edu Heather Harrell harrehe@medicine.ufl.edu (Provided progress note examples and has many more)