Download

1 / 14
200 likes | 799 Views
PCOS. Valerie Robinson, DO. PCOS. Polycystic Ovarian Syndrome (PCOS) is a disorder that causes menstrual and ovulation irregularities, androgen excess, and infertility. Polycystic ovaries are found on ultrasound. PCOS is often found in an infertility work-up.

E N D
PCOS Valerie Robinson, DO
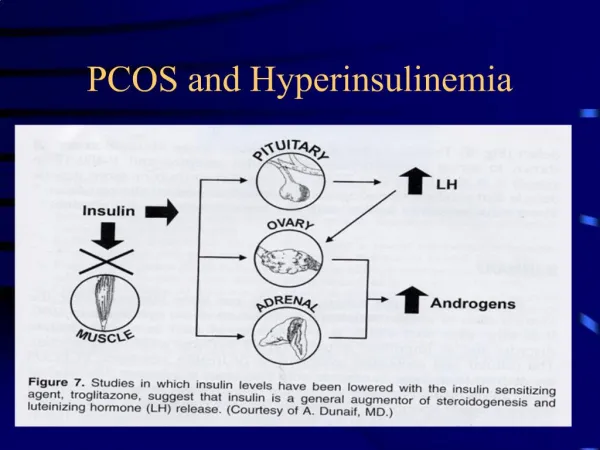
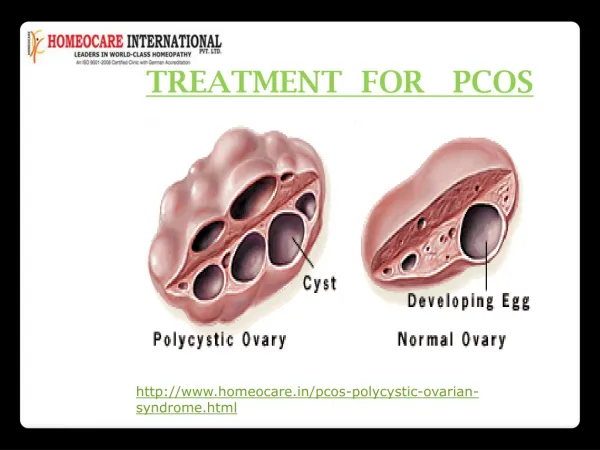
PCOS • Polycystic Ovarian Syndrome (PCOS) is a disorder that causes menstrual and ovulation irregularities, androgen excess, and infertility. Polycystic ovaries are found on ultrasound. • PCOS is often found in an infertility work-up. • Intraovarian androgen excess excessive growth of small follicles and hinders maturation of a dominant follicle anovulation • Other common findings include obesity and insulin resistance
PCOS • Prevalence is 6-8% in the general population • Onset is usually during or soon after puberty • Polycystic ovaries may not develop until two or more years after menarche • Increased incidence is found in the following • Use of anti-epileptic drugs - specifically valproate • Mexican-American • First degree family history – risk is 20-40% • History of premature adrenarche • Diabetes - type 1, type 2, or gestational • Infertility • Risk factors • First degree relative with polycystic ovaries • First degree relative with hyperandrogenism • Mother with PCOS • Father or Mother with metabolic syndrome • Congenital virilization (MCC is congenital adrenal hyperplasia) • Insulin resistance or hyperinsulinemia
Symptoms • Menstrual dysfunction • Oligo- or anovulation Infertility • Oligo- or amenorrhea with irregular cycles • Adolescents may have delayed menarche • May begin regular menses and develop irregularity • Increased risk of endometrial hyperplasia/cancer. Oligoovulation results in decreased progesterone secretion. Relative lack of progesterone leads to chronic unopposed estrogen exposure. • Ovarian abnormalities • Multiple small antral and pre-antral follicles in the periphery • Follicle growth is arrested in antral stage • Increased thickness of stroma • Ovarian cortex is thickened and sclerotic
Symptoms - continued • Increased risk of metabolic syndrome • Obesity, usually central • Insulin resistance and hyperinsulinemia • Acanthosisnigricans • Pseudo-acromegaly • Diabetes type 1 or 2 • Dyslipidemia • Hyperandrogenism • Hirsutism • Acne • Male-Pattern balding • Hyperpituitarism • Acromegaly • Hyperprolactinemia
Symptoms – continued • Increased likelihood of depression and anxiety • Increased risk of NASH • Increased risk of CAD
Diagnostic criteria • National Institutes of Health (NIH) 1990 criteria: irregular menses, biochemical and/or clinical hyperandrogenism.Other causes of hyperandrogenismexcluded. • Rotterdam 2003 criteria (requires two out of three of the following): oligo- and/or anovulation, clinical and/or biochemical hyperandrogenism, polycystic ovaries by ultrasound. Other causes of hyperandrogenism excluded. • Exclude congenital adrenal hyperplasias, androgen-secreting tumors, Cushing's syndrome, hyperprolactinemia, steroid use.
Diagnosis • Menstrual history • Physical exam • Transvaginal Ultrasound • 8-10 small follicles surrounding thickened stroma: “String of Pearls” • Rotterdam Criteria: 12 or more follicles 2-9mm, or ovarian volume of >10mL • As a lone finding, polycystic ovaries is insufficient for diagnosis • Hormone abnormalities: non-diagnostic findings • Some women may have increased LH, decreased FSH, increased prolactin • Women with PCOS should be screened for depression, glucose intolerance, dyslipidemia, HTN
Diagnosis - continued • Serum HCG to rule out pregnancy in amenorrhea • In high risk women or with virilization, testing may be needed to rule out other uncommon causes of hyperandrogenism. • Morning serum 17-hydroxyprogesterone in the follicular phase • Serum testosterone • Serum prolactin and TSH
Treatment – symptomatic • Obesity • Weight loss: diet and exercise, bariatric surgery • Insulin-lowering agents: metformin • Hyperandrogenism • Estrogen/Progesterone OCPs, also provide endometrial protection • Antiandrogen after 6 months • Spironolactone (if not planning conception), finasteride • GnRHagonist (leuprolide) suppresses ovarian function • Dyslipidemia • Statins • Fibrates • NASH • Weight loss • Metformin • Anovulation • Weight loss • Clomid • Metformin
Treatment – by category • Weight loss: • Reduces androgenism, improves ovulation, and increases chance of planned pregnancy. • Insulin-lowering agents • Clomiphine • Increases chances of ovulation • Metformin • Decreases insulin resistance and hyperinsulinemia, increases insulin sensitivity decreased androgens. May promote ovulation • Aromatase inhibitor • Induces ovulation • Gonadotropins – • Increases chances of ovulation • Surgery • We no longer use wedge resection • We do occasionally use “ovarian drilling” to induce ovulation
References • Ricardo Azziz, MD et al. “Epidemiology and pathogenesis of the polycystic ovary syndrome in adults.” UpToDate. Updated 7/17/12 • Robert L Barbieri, MD, David A Ehrmann, MD et al. “Clinical manifestations of polycystic ovary syndrome in adults.” UpToDate. Updated 8/3/12. • Robert L Barbieri, MD David A Ehrmann, MD et al. “ Diagnosis of polycystic ovary syndrome in adults.” UpToDate. Updated 3/9/12. • Robert L Barbieri, MD David A Ehrmann, MD et al. “Treatment of polycystic ovary syndrome in adults.” UpToDate. Updated 9/20/12.
References – continued • Robert L Rosenfield, MD et al. “Clinical features and diagnosis of polycystic ovary syndrome in adolescents.” UpToDate. Updated 6/15/11. • Robert L Rosenfield, MD et al. “Definition, pathogenesis, and etiology of polycystic ovary syndrome in adolescents.” UpToDate. Updated 6/15/11. • Robert L Rosenfield, MD et al. “Treatment of polycystic ovary syndrome in adolescents.” UpToDate. Updated 6/16/11. • Figures http://www.advancedfertility.com • Figures https://ufandshands.org/polycystic-ovary-syndrome