Download
1 / 29
330 likes | 493 Views
Liver It is the largest gland in the body. Its functions are production of bile pigments from the hemoglobin of worn-out red blood corpuscles and secretes bile salts these together are conveyed to the duodenum by the biliary ducts. Also, it synthesizes heparin

E N D
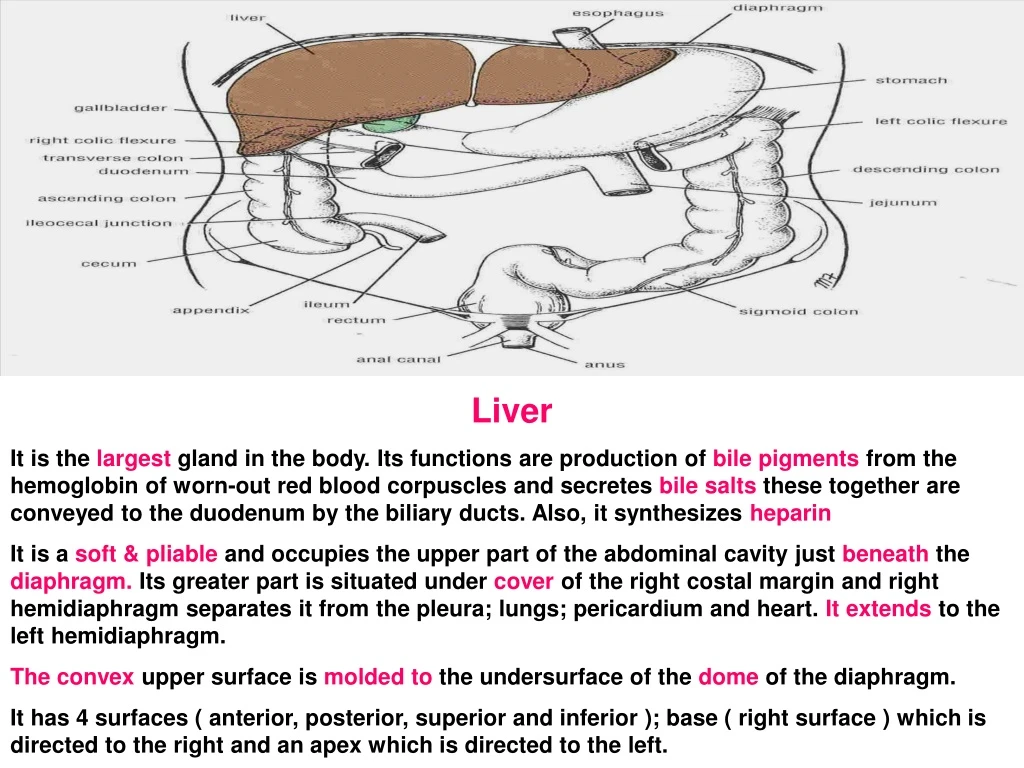
Liver It is the largest gland in the body. Its functions are production of bile pigments from the hemoglobin of worn-out red blood corpuscles and secretes bile salts these together are conveyed to the duodenum by the biliary ducts. Also, it synthesizes heparin It is a soft & pliable and occupies the upper part of the abdominal cavity just beneath the diaphragm. Its greater part is situated under cover of the right costal margin and right hemidiaphragm separates it from the pleura; lungs; pericardium and heart. It extends to the left hemidiaphragm. The convex upper surface is molded to the undersurface of the dome of the diaphragm. It has 4 surfaces ( anterior, posterior, superior and inferior ); base ( right surface ) which is directed to the right and an apex which is directed to the left.
1 Bare area cudate fundus 2 stomach 2nd Lesser omentum Pylorus Transverse colon Renal duodenal R. R Colic The posteroinferior or visceral surface is irregular in shape. It lies in contact with the abdominal part of the esophagus (1 ); stomach; duodenum; right colic flexure; right kidney; suprarenal gland ( 2 ) and the gallbladder. The porta hepatis ( hilum of the liver ) lies on this surface. It lies between the caudate & quadrate lobes. The right lobe is divided into a quadrate lobe and a caudate lobe by the presence of the gallbladder; the inferior vena cava; the fissure for the ligamentum teres; and the fissure for the ligamentum venosum. These 2 fissures meet each other at the left end of porta hepatis. Functionally, the caudate & quadrate lobe are parts of the left lobe. N.B. the caudate lobe lies above opening of lesser sac ( tuber omentale ) and in front of the superior recess of the lesser sac.
The liver is divided into right & left lobe by the attachment of the peritoneum of the falciformligament. The liver is completely surrounded by a fibrous capsule but only partially covered by peritoneum. The bare area; fossa for gall bladder; fossa for inferior vena cava and lines of attachment of various ligaments not covered with peritonum. The liver is made up of liver lobules. The central vein of each lobule is a tributary of the hepaticveins. In the spaces between the lobules are the portal canals which contains branches of the hepatic artery ; tributary of a bile duct and portal vein. The arterial and venous blood passes between the liver cells by means of sinusoids and drains into the central vein.
In the porta hepatis lie the right & left hepatic ducts; the right & left branches ofthe hepatic artery; the portal vein and sympathetic & parasympathetic nerve fibers and a few hepatic lymph nodes which drain the liver and gall bladder and send their efferent vessels to the celiac lymph nodes. The upper part of the edge of the lesser omentum is attached to the margin of the porta hepatis.
Lesser omentum: It connects the lesser curvature of the stomach & duodenum to the fissure of the ligamentum venosum and the portahepatis on the under-surface of the liver. Its free border is formed where the 2 layers are continuous. It forms the anterior boundary of the opening to the lesser sac. It contains along the lesser curvature the right & left gastric vessels. At the free border the hepatic artery & bile duct anteriorly and portal vein posteriorly.
Falciform ligament It is a sickle- shaped fold which connects the liver to the diaphragm and anterior abdominal wall. It has 3 borders 1- Convex border which is attached to the diaphragm & anterior abdominal wall down to the umbilicus in the median plane. 2- concave border which is attached to anterior & upper surfaces of the liver between the right & left lobes. On the upper surface of the liver the 2 layers of the ligament separate and the right one joins the superior layer of the coronary ligament, while the left layer joins the anterior layer of the left triangular ligament. 3- Free border which extends from the umbilicus to the notch for ligamentum teres at the inferior border of the liver. It contains the ligamentum teres ( obliterated left umbilical vein ) and paraumbilical veins. At the free border , the 2 layers of the ligament are continuous with each other.
Coronary ligament It consists of 2 layers which enclose between them the bare area of the liver. The superior layerconnects the right lobe of the liver with the diaphragm and is continuous medially with the right layer of the falciform ligament. It is continuouslaterally with the anterior layer of the right triangular ligament. The inferior layerconnects the right lobe of the liver either with the diaphragm or right hepato-renal ligament. It is continuouslaterally with the posterior layer of the right triangular ligament. It is attachedmedially to the lower part of groove for IVC; right margin & upper border of the caudate lobe of the liver. Its ends join posterior layer of lesser omentum at the upper end of the fissure for ligamentum venosum.
Right triangular ligament It connects the upper surface of the right lobe of the liver with the diaphragm.Medially, Its anterior & posterior layers are continuous with superior & inferior layers of coronary ligament. Left triangular ligament It connects the upper surface of the left lobe of the liver with the diaphragm.Medially, Its anterior layer is continuous with the left layer of falciform ligament. Its posterior layer joins anterior layer of lesser omentum at the upper end of the fissure for ligamentum venosum. N.B. The previous ligaments are called hepatophrenic ligaments.
Relations Anteriorly: Diaphragm; right & left costal margins; right and left pleura and lower margins of bothlungs; xiphoid process and anterior abdominal wall in the subcostal angle. Posteriorly: Diaphragm; right kidney; hepatic flexure of the colon; duodenum; gallbladder; inferior venacava; esophagus and fundus of the stomach.
The ligamentum teres passes into a fissure on the visceral surface of the liver and joins the left branch of the portal vein in the porta hepatis. The ligamentum venosum ( a fibrous band that is a remains of the ductus venosus ) is attached to the left branch of the portal vein and ascends in a fissure on the visceral surface of the liver to be attached above to the inferior vena cava. In the fetus, oxygenated blood is brought to the liver in the left umbilical vein ( ligamentum teres ). The greater proportion of the blood bypasses the liver in the ductus venosus ( ligamentum venosus ) and joins the inferior vena cava. At birth, the umbilical vein and ductus venosus close and become fibrous cord
Blood Supply The hepatic artery, a branch of the celiac artery, divided into right & left terminal branches that enter the porta hepatis. The portal vein divided into right & left terminal branches that enter the portahepatisbehind the arteries. The hepatic veins ( 3 or more ) emerges from the posterior surface of the liver and drain into the inferior vena cava.
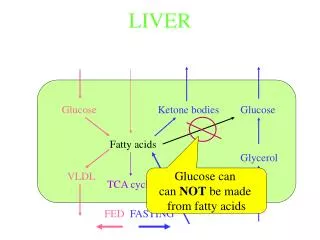
Blood Circulation through the Liver: The blood vessels conveying blood to the liver are the hepatic artery ( 30% ) and portal vein ( 70 % ). The hepatic artery brings oxygenated blood to the liver and the portal vein brings venous blood rich in the products of digestion which have been absorbed from the gastrointestinal tract. The arterial and venous blood is conducted to the central veins drain into the right & left hepatic veins and these leave the posterior surface of the liver and open directly into the inferior vena cava.
Lymph Drainage The liver produces large amount of lymph- about one third to one half of all body lymph. The lymph vessels leave the liver and enter several lymph nodes in the porta hepatis. The efferent vessels pass to the celiac nodes. A few vessels pass from the bare area of the liver through the diaphragm to the posterior mediastinal lymph nodes. Nerve Supply Sympathetic and parasympathetic nerves form the celiac plexus. The anterior vagal trunk gives rise to a large hepatic branch which pass directly to the liver.
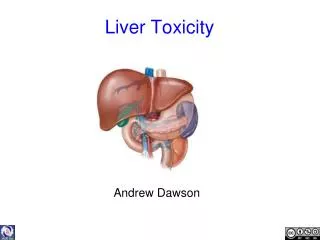
Clinical Notes 1- Liver Trauma: It is a soft; friable structure enclosed in a fibrous capsule. Fractures of the lower ribs or penetrating wounds of the thorax or upper abdomen are common causes of liver injury. Blunt traumatic injuries from automobile accidents are also common and severe hemorrhage accompanies tears of this organ. The bile ducts; hepatic arteries and portal vein are distributed in a segmentalmanner. So, appropriate ligation of these structures allows the surgeon to remove large portions of the liver in patients with severe traumatic laceration of the liver or with liver tumor. Even large localized carcinomatous metastatic tumors have been successfully removed. 2- subphrenic Spaces: An abnormal accumulation of gas or fluid is necessary for separation of peritoneal surfaces. The anterior surface of the liver is normal dull on percussion. Perforation of a gastric ulcer is often accompanied by a loss of the liver dullness caused by accumulation of gas over the anterior surface of the liver and in the subphrenic spaces.
Greater sac It is the space which is exposed when the anterior abdominal wall is cut. It is divided by the greater omentum; transverse colon and transverse mesocolon 1- Upper anterior part ( supracolic part ) above transverse colon. 2- lower posterior part ( infracolic part)below transverse colon. The 2 parts are continuous with each other at the lateral borders of the greater omentum. Supracoliccompartment lies above the transverse colon and below the diaphragm. It is divided by hepatophrenic ligaments (falciform ligament; coronary ligament and right & left triangular ligaments ) into : 1- Right & leftsubphrenic recesses. 2- Hepatorenal recess between the diaphragm and right kidney. 3- Left subhepatic space ( omental bursa).
Subphrenic spaces These are potential spaces only, and the peritoneal surfaces are in contact. The right & left anterior subphrenic spaces lie between the diaphragm and the liver on each side of the falciform ligament. The right posterior subphrenic space lies between the right lobe of the liver ; the right kidney and the right colic flexure.
A patient with a subphrenic abscess or collections of blood under the diaphragm may complain of pain over the shoulder due to irritation of the parietal diaphragmatic peritoneum. The skin of the shoulder is supplied by the supraclavicualr nerves ( C3, C4 ). To avoid the accumulation of infected fluid in the subphrenic spaces and to allow this fluid to gravitate downward into the pelvic cavity where the rate of toxin absorption is slow. The patient must sit up in bed with the back at an angle of 45°. Two extraperitoneal spaces in the subphrenic region may become the site of localized infection. 1- Right extraperitoneal space which lies between the 2 layers of the coronary ligament ( bare area ) of the liver and the diaphragm. 2- Left extraperitoneal space which comprises the extraperitoneal connective tissue around the left suprarenal gland and the upper pole of the left kidney.
The liver lies under cover of the lower ribs and most of its bulk lies on the right side. In infants, until about the end of the 3rd year, the lower margin of it extends 1 or 2 fingerbreadths below the costal margin. In adult who are obese or has a well developed right rectus abdominismuscle, the liver is not palpable. In a thin adult, the lower edge of the liver may be felt a fingerbreadthbelow the costal margin. It is easily felt when the patient inspires deeply and the diaphragm contracts and pushes down the liver. The fundus of the gallbladder lies opposite the tip of the 9th costal cartilage. This area is where the lateral edge of the right rectus abdominis muscle crosses the costal mergin.
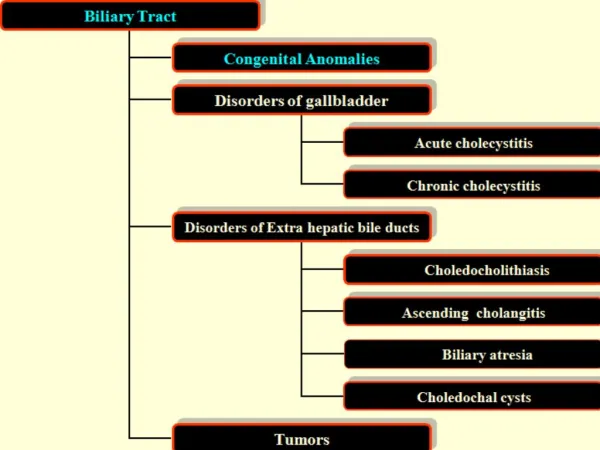
Bile Ducts Bile is secreted by the liver cells at a constant rate of about 40 ml per hour. The bile is stored and concentrated in the gallbladder. Then ,it delivered to duodenum. The bile ducts consists of the right & left hepatic ducts; common hepatic duct; gallbladder; cystic duct and bile duct. The right hepatic duct drains the right lobe of the liver and the left duct drains the left lobe ; caudate and quadrate lobes. The right & left hepatic ducts emerge from the right & left lobes of the liver in theporta hepatis. They unite after a short distance to form the common hepatic duct which is about 1.5 inch (4 cm ) long. It descends within the free margin of the lesser omentum. It is joined on the right side by the cystic duct from the gallbladder to form the bile duct.
Cystic duct It is about 1.5 ( 3.8 cm ) long and connects the neck of the gallbladder to the common hepatic duct to form the bile duct. It is usually S shaped and descends in the right free margin of the lesser omentum. The mucous membrane of the cystic duct is raised to form a spiralfold that is continuous with a similar fold in the neck of the gallbladder. These folds is called spiral valves which keep the lumen constantly open.
Common Bile Duct It is about 3 inch ( 8 cm ) long. In first part of its course , it lies in the right free margin of the lesser omentum in front of the opening into the lesser sac. Here , it lies in front of the right margin of the portal vein and on the right side of the hepatic artery. In the second part of its course, it is situated behind the 1st part of the duodenum to the right of the gastroduodenal artery. In the third part of its course , it lies in a groove on the posterior surface of the head of the pancreas. Here , the bile duct comes into contact with the main pancreatic duct.
The bile duct ends below by piercing the medial wall of the 2nd part of duodenum about halfway down its length. It is joined by the main pancreatic duct and together they open into a smallampulla in the duodenal wall called the hepatopancreatic ampulla ( ampulla ofVater). This ampulla opens into the lumen of the duodenum by means of a small papilla ( the major duodenal papilla ). The terminal parts of both ducts and the ampulla are surrounded by circular muscle ( smooth ) known as the sphincter of the hepatopancreatic ampilla ( sphincter of Oddi) Occasionally, the bile and pancreatic ducts open separately into the duodenum.
Gallbladder It is a pear shaped sac lying on the undersurface of the liver. It has a capacity of 30 to 50 ml and stores bile which it concentrates by absorbing water. It is divided into fundus; body and neck. The fundusis rounded and projects below the inferior margin of the liver where it comes in contact with the anterior abdominal wall. The body lies in contact with the visceral surface of the liver and is directed upward; backward and to the left. The neckbecomes continuous with the cystic duct which turns into the lesser omentum to join the right side of the common hepatic duct to form the bile duct.
Relations : Anteriorly:The anterior abdominal wall and the inferior surface of the liver. Posteriorly: The transverse colon and the 1st and 2nd parts of the duodenum. The peritoneum completely surrounds the fundus of the gallbladder and binds the body and the neck to the visceral surface of the liver.
Function of the Gallbladder When digestion is not taking place, the sphincter of Oddi remains closed and bile accumulate in the gallbladder which concentrates bile; stores bile; absorbs bile salts; keeping the bile acid; excretes cholesterol and secretes mucus. The mucous membrane is thrown into permanent folds that unite with each other giving the surface a honeycombed appearance. The columnar cells lining the surface have microvilli on their free surface. Bile is delivered to the duodenum as a result of contraction and partial emptying of the gallbladder. This mechanism is initiated by the entrance of fatty foods into the duodenum. The fat causes release of the hormone cholecystokinin from the mucous membrane of the duodenum. The hormone then enters the blood causing the gallbladder to contract. At the same time the, the smooth muscle around the distal end of the bile duct and the ampulla is relaxed , thus allowing the passage of concentrated bile into the duodenum. The bile salts in the bile are important in emulsifying fat in the intestine and assisting with its digestion and absorption.
Blood Supply The cystic artery which is a branch from the right hepatic artery. It supplies the gallbladder. The cystic vein drains directly into the portal vein. Several small arteries & veins also run between the liver and gallbladder. Nerve Supply Sympathetic & parasympathetic vagal fibers form the celiac plexus. The gallbladder contracts in response to the hormone cholecystokinin which is produced by the mucous membrane of the duodenum on the arrival of fatty food from the stomach. Lymph Drainage It drains into a cystic lymph node situated near the neck of the gallbladder. From this, the lymph vessels pass to the hepatic nodes along the course of the hepatic artery and then to the celiac nodes.
Clinical Notes 1- Gallstones They are usually asymptomatic. Also, they can give rise to gallbladder colic or produce acute cholecystitis. 2- Acute Cholecystitis It produces discomfort in the right upper quadrant or epigastrium. Inflammation of the gallbladder may cause irritation of the subdiaphragmatic parietal peritoneum which is supplied in part by the phrenic nerve ( C 3,4 and 5 ) This may give rise to referred pain over the shoulder because the skin in this area is supplied by the supraclavicular nerves ( C 3 and 4 ).
3- Biliary Colic It is usually caused by spasm of the smooth muscle of the wall of the gallbladder to expel a gallstone. Afferent nerve fibers ascendsthrough the celiac plexus and the greater splanchnic nerves to the thoracic segments of the spinal cord. Referred pain is felt in the right upper quadrant or the epigastrium ( T 7; 8 and 9 dermatomes ). Obstruction of the biliary ducts with a gallstone or by compression by a tumor of the pancreas results in backup of bile in the ducts and development of jaundice. The impaction of a stone in the ampulla ofVater may result in the passage of infected bile into the pancreatic duct producing pancreatitis. Gallstones have been known to ulcerate through the gallbladder wall into the transverse colon or the duodenum. They may passed naturally per rectum. But, they may be held up at the ileocecal junction producing intestinal obstruction.
4- Cholecystectomy & Arterial supply to Gallbladder The pattern of arterial supply to gallbladder must be observed before cholecystectomy operation. To avoid legation of the arteries with the common hepatic duct or the main bile duct . 5- Gangrene of the gallbladder It is rare because it is receives cystic artery from the right hepatic artery and also small branches from the visceral surface of the liver. Sonograms is used to demonstrate the gallbladder.