Download
1 / 32
320 likes | 523 Views
Digestive System. Chapter 23. Overview. Alimentary canal or gastrointestinal ( GI ) tract Accessory digestive organs Food moved by peristalsis Regulated by sphincters Processing time varies. Digestive Processes. Ingestion : act of eating Propulsion : moving food through GI tract

E N D
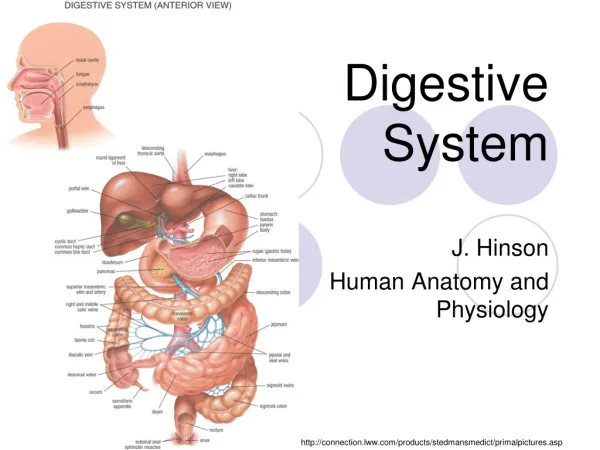
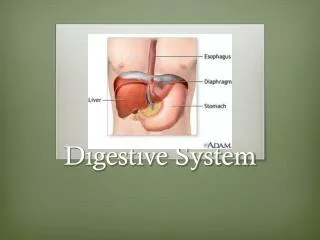
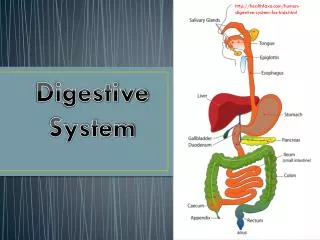
Digestive System Chapter 23
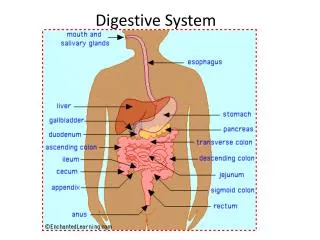
Overview • Alimentary canal or gastrointestinal (GI)tract • Accessory digestive organs • Food moved by peristalsis • Regulated by sphincters • Processing time varies
Digestive Processes • Ingestion: act of eating • Propulsion: moving food through GI tract • Deglutition and peristalsis • Digestion: break down of food • Mechanical uses chewing, mixing, and churning • Chemical uses enzymes • Absorption: nutrients, vitamins, minerals, and H2O into blood • Defecation: elimination of undigested materials
Peritoneum • Serous membrane of the abdominal cavity • Review: what are components? • Mesenteries fuse parietal to visceral • Routes for vascular, lymph, and nervous supply to viscera • Holds organs in place and stores fat • Retroperitoneal organs lie outside peritoneum • Includes pancreas, kidneys, parts of large intestine • Intraperitoneal organs stay w/i cavity • Includes stomach, small and parts of large intestine, liver • Blood supply • Celiac trunk and mesenteric arteries to digestive viscera • Hepatic portal to liver for storage and processing http://www.vivo.colostate.edu/hbooks/pathphys/misc_topics/peritoneum.html
Basic Histology • 4 tunics line entire GI tract • Mucosa from mouth to anus • Epithelium is simple columnar w/goblet cells • Lamina propria is areolar CT a nd MALT (chpt 20 review) • Muscularis mucosae is smooth muscle • Submucosa • Areolar CT, blood, lymph, and nerves • Muscularisexterna • Smooth muscle in circular (inner) and longitudinal (outer) layers • Serosa (visceral peritoneum) • Areolar CT w/ simple squamous layer • Predominant tissue type facilitates processing role • Fig 23.6
Oral Cavity: Mouth • Stratified squamous epithelium • Lips (orbicularis oris) and cheeks (buccinators) • Mastication and forming words/pronunciation • Palate • Hard (palatine process of maxilla and palatine bones) • Soft (skeletal muscle) with hanging uvula • Tongue (skeletal muscle) • Food manipulation (bolus), taste, and speech production • Tastebuds • Filiform papillae: not tastebuds, roughen tongue surface • Fungiform papillae: mushroom shaped w/ tastebuds on top • Circumvallate papillae: circular w/tastebuds on sides
Oral Cavity: Salivary Glands • Parotid, submandibular, sublingual, and buccal • Serous and mucus cells produce saliva components • Saliva • Lysozymes, IgA, and defensins cleanse and protects mouth from microorganisms • Mucin and water (97 – 99%) to moisten and dissolve food • Salivary amylase breaks down carbs • Control • Intrinsic continuously secrete to keep mouth moist • Extrinsic in response to food; sight, smell & thought too • SNS inhibits causing dry mouth, xerostomia • Halitosis and caries from food particles accumulating and bacteria flourishing
Oral Cavity: Teeth • Chew, tear and grind food to initiate breakdown • Deciduous, or milk teeth, form 1° dentition (20) • Permanent teeth from permanent dentition (32*) • Types • Incisors cut and nip (8, 2 pairs top and bottom) • Canines tear and pierce (4, 1 pair top and bottom) • Premolars grinding and crushing (8, 2 pairs top and bottom) • Molars see premolars (12, 3*pairs top and bottom) • Dental formula • (__I x __C x __M / __I x __C x __M) x 2 = • Impacted teeth when remain in jaw
Oral Cavity: Teeth (cont.) • Crown exposed above gingiva • Covered in enamel, hardest material in body • No mitotic activity to fix cracks and decay • Overlays bone-like dentin • Root anchored in jaw by periodontal ligament • Gomphosis in alveolar margin • Number varies by tooth type and location • Covered in cementum, calcified CT • Pulp cavity become root canal w/ apical foramen • Damage to nerve and blood supply facilitates infection • Root canal therapy to sterilize before filling
Tooth and Gum Disease • Caries or cavities when enamel and dentin decay • Dental plaque adheres and acidity increases • Ca2+ salts removed, organics dissolved by bacteria • Brushing and flossing daily prevent • Calculus, or tarter causes gingiva separation • Gingivitis, an early indication, causes bleeding and swelling • Periodontal disease when calculus untreated • Immune system attacks bacteria and periodontal ligaments • Osteoclast activity increased • Research links w/increase risk of heart attack and stroke
Pharynx • Oropharynx laryngopharnx • Food and fluids to esophagus • Air to trachea • Lined w/ stratified squamous and goblet cells • Skeletal muscle layers for swallowing • Inner longitudinal • Outer circular pharyngeal constrictors
Esophagus • Laryngopharynx esophageal sphincter esophageal hiatus cardiac orifice gastroesophageal sphincter • Heartburn when GE sphincter not tightly closed/leaks • Histology • Mucosa w/ strat. squ. sim. colum. • Folds w/o food that flatten w/ food • Submucosa w/ mucus glands to aid passage • Muscularisexterna w/ skeletal skeletal & smooth smooth • Fibrous CT fibrous adventitia instead of serosa
Mouth to Esophagus Digestion • Mouth ingests • Mastication uses teeth and tongue to start mechanical digestion • Food and structure mov’t influences • Salivary amylase starts chemical digestion of carbs • Tongue forms bolus for deglutition • Tongue pushes to oropharynx in buccal phase (voluntary) • Esophageal sphincter constricts • Pharyngeal-esophageal phase (involuntary) • Uvula and epiglottis protection triggered • Esophageal sphincter relaxes • Peristalsis moves bolus down esophagus • Gastroesophagealspincter relaxes then constricts • Prevents chyme escape
Stomach • Chemical breakdown of proteins • Regions • Cardia • Fundus • Body • Pyloric region (antrum, canal, and sphincter) • Mesenteries (greater and lesseromentums) at respective curvatures • Rugaeseen when empty, allow distension
Stomach: Microscopic Anatomy • Muscularisexternaw/ 3rd oblique layer to break food and push to SI • Mucosa • Simple columnar epithelia w/ goblet cells • Insoluble alkaline mucus layer w/ bicarbonate fluid below • Protects stomach from acid and enzyme digestion • Invaginates into gastric pits leading to gastric glands that produce gastric juices, mucus, and gastrin • Pits are primarily mucus cells • Glands vary w/ region
Gastric Glands • Mucus neck cells produce acidic mucus • Function not understood • Parietal cells secrete H+ and Cl- ions HCl • Acidity (pH ~ 2) denatures proteins, kill bacteria, and digest cellulose • Intrinsic factor production: B12 absorption for RBC production • Chief cells produce pepsinogen pepsin • HCl initiates, but pepsin maintains (positive feedback) • Enteroendocrine cells release chemical messengers • Histamine, gastrin, serotonin, endorphins, cholecystokinin (CCK), and somatostatin
Protecting the Stomach • Insoluble mucus layer on surface • Bicarbonate ions (HCO3-) • Tight junctions b/w epithelial cells • H+ and Cl- ions secreted separately • Epithelial replaced ~ 3 – 6 days • Gastric ulcers form when mechanisms fail • Chronic can rupture stomach • Helicobacter pylori usually responsible
Controlling Gastric Secretion • Cephalic (reflex) phase before food entry • Smell, taste, thought, or sight excites • Depression or lack of appetite suppress • Gastric phase once food enters stomach • Stretch receptors signal ACh to increase gastric juices • Peptides, caffeine, and high pH stimulate gastrin (HCl) release • Low pH, emotions, and SNS inhibit gastrin • Intestinal phase once food enters duodenum (SI) • W/ low pH and food stimulates intestinal gastrin release • Distension and prolonged low pH inhibit CN X, activate SNS to tighten pyloric sphincter, and release inhibiting hormones • Fig 23.17
Controlling Mobility and Emptying • Peristalsis pushes to pyloric for mixing before retropulsion pushes back • Chyme squirts through pyloric valve w/ each cycle • Duodenum monitoring tightly coupled • Inhibiting hormones from intestinal phase (previous) • Carb rich chyme moves quickly, but fat rich chyme slower for digestion • Vomiting or emesis • Fig 23.30
Small Intestine (SI) • Digestion finishes and nutrient absorption occurs • 3 subdivision w/ no clear external distinctions • Duodenum (retroperitoneal) • Receives chyme from pyloric sphincter • Hepatopancreaticampulla where bile and pancreatic duct join (sphincterofOddi controls) • Jejunum (mesentery support) • Ileum (mesentery support) • Ileocecal valve at LI junction
Small Intestine: Microscopic Anatomy • Mucosa and submucosa form plicaecirculares • Simple columnar mucosa folds into villi • Lacteal, artery, and vein w/i • Intestinal crypts b/w • Intestinal juice, Panethcells, and new cells • PM of mucosa cells form microvilli (brush border) • Enzymes finalize carb and protein digestion • Increase SA for absorption • Submucosa variations throughout SI region • Intestinal crypts decrease • Goblet cell number increases • Peyer’s patches (MALT) increase • Brunner’s glands (HCO3- mucus) in duodenum only • Muscularisexterna • Duodenum w/ adventitia (retroperitoneal)
Liver • Right, left, caudate, and quadratelobes • Falciformligament is the mesentery • Separates R & L and suspends liver from diaphragm • Ligamentteres is remnant of umbilical vein • Lesseromentum connects curvature to liver • Hepatic artery, vein, and portal vein • Hepaticducts hepatic duct commonbileduct • Hepatitis and cirrhosis
Liver: Microscopic Anatomy • Hexagonal liver lobules are functional units • Hepatocytes arranged around a central vein • Portal triads at each corner • Bile duct, hepatic artery, and hepatic portal vein • Liver sinusoids (capillaries) b/w • Kupffer cells
Gallbladder • Stores and concentrates liver produced bile • Hepatic duct cystic duct storage • Cystic duct common bile duct sphincter of Oddirelease • Bile • Alkaline solution to emulsify lipids • Facilitate fat and cholesterol absorption • Bile salts recycled in illeum back to liver (hepatic portal vein) • Bilirubin, chief pigment, absorbed in liver and released in bile • Gallstones from cholesterol crystallization • Jaundice when bile pigments accumulate in skin from blockage
Pancreas • Retroperitoneal organ • Acinar cells produce digestive enzymes that breakdown all foodstuffs • Pancreatic duct joins common bile to drain to duodenum (where specifically?) • Islets of Lagerhansproduce insulin and glucagon
Pancreatic Juice • Water based solution of enzymes and HCO3- • Neutralize chyme (pH ~ 2 vs pH ~ 8) • Optimal pH for enzymes • Enzymes hydrolyze monomers • Inactive proteases • Active amylases, lipases, and nucleases
Accessory Secretion Regulation • Neural (CN X) and hormonal (CCK & secretin) control • CCK released w/ fatty chyme presence • Gallbladder contract and sphincter of Oddi relax • Vagus nerve weakly • Bile and pancreatic juice (enzyme rich) secreted • Secretin released w/ HCl presence • HCO3- rich pancreatic juice release • Bile salt presence stimulates more bile release • Positive feedback
Large Intestine • Absorb water & vitamins and eliminate feces • Tone of teniae coli create pouch-like haustra • Divisions • Cecum • Appendix (MALT) • Appendicitis when blocked and bacterial growth • Ascending and descending colon are retroperitoneal • Transverse and sigmoid colon w/ mesocolons • Rectum w/ rectal valves to separate feces and gas • Anal canal w/ internal and external sphincters • Imbalances • Diarrheavsconstipation
Large Intestine: Microscopic Anatomy • Mucosa • Simple columnar except anal canal (strat. squa.) • No folds, villi, or digestive enzyme cells • Thicker w/ deeper crypts and more goblet cells • Bacterial flora • Enter via anus or survive SI • Functions • Breakdown indigestible carbs (cellulose) • Release gases from breakdown • Synthesize vitamins B and K • Generally peaceful existence • Irritable bowl syndrome (disease) when not
Nutrient Digestion • Catabolic process of hydrolysis • Carbohydrates • Amylases (salivary and pancreatic) • Brush border enzymes (dextrinase, lactase, maltase, sucrase) • From villi to liver in hepatic portal vein • Proteins • Pepsin in stomach (pepsinogen + HCl) • Brush border peptidases (amino-, carboxy-, di) • Pancreatic proteases (trypsin, chymotrypsin, carboxypeptidase) • Lipids • Bile sales emulsifies fats to expose triglycerides • Pancreatic lipase forms glycerol and FA’s • Nucleic acids • Brush border enzymes (nuclesidases and phosphotases) • Pancreatic nucleases (deoxy- and ribonucleases) • Fig 23.32
Nutrient Absorption • Carbohydrates • Glu and gal: active transport (w/ Na+) to epithelium then facilitated diffusion to capillaries • Fru: only facilitated diffusion • Proteins • See glucose and galactose above • Inefficient in newborns = food allergies as endocytized whole proteins ‘seen’ as antigens; allow IgA from breast milk into blood • Lipids • Monomers bind w/ bile salts = micelles to reach epithelium for diffusion • Chylomicrons in epi. when reassembled water soluble lacteal absorb • Nucleic Acids • See glucose and galactose above
Nutrient Absorption (cont.) • Vitamins • Fat soluble see lipids previous; need to eat w/ • Water soluble by diffusion, active, or passive transport • Electrolytes • Anions move w/ Na+ gradient (glucose & glactose) • Iron and Ca2+ regulated by body needs • K+ related to water volume/absorption • Water • 95% in SI, rest in LI • Bidirectional, but net osmosis w/ [gradient] from active solute absorption