Download
1 / 74
750 likes | 908 Views
Non-Cognitive Diagnostic Assessment of TBI/Sports Concussion. Barry D. Jordan M.D., M.P.H. Director, Brain Injury Program Burke Rehabilitation Hospital Associate Professor Clinical Neurology Weill Medical College of Cornell University Former Chief Medical Officer

E N D
Non-Cognitive Diagnostic Assessment of TBI/Sports Concussion Barry D. Jordan M.D., M.P.H. Director, Brain Injury Program Burke Rehabilitation Hospital Associate Professor Clinical Neurology Weill Medical College of Cornell University Former Chief Medical Officer New York State Athletic Commission
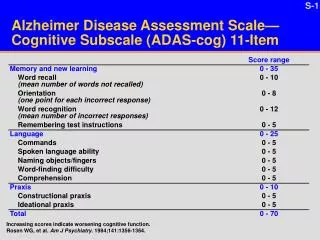
Concussion Evaluation • Neurodiagnostic Testing • Neuropsychological Testing • Neuroimaging • Biomarkers of brain injury • Objective Balance Assessment • Electrophysiological testing • Genetic testing • Eye tracking techniques
Non-computerized cognitive assessment Standardized Assessment of Concussion (SAC) Sport Concussion Assessment Tool 2 (SCAT 2) McGill On-Field Concussion Evaluation Maddocks Score Military Acute Concussion Evaluation (MACE) Standard pencil paper neuropsychological testing
Neuroimaging • Traditional structural neuroimaging • CT • MRI • Newer structural neuroimaging • DTI • Functional and metabolic scanning • PET • SPECT • fMRI • MRS • NIRS
Diffusion anisotropy: fiber tract integrity CST damaged fiber tract healthy fiber tract decreased directional dependence of water diffusion strong directional dependence of water diffusion
Fiber Tractography in TBI • Anterior corona radiata and genu of CC • Uncinate fasiculus • Cingulum bundle and body of CC • Inferior longitudinal fasciculus
a b d c Figure 2. Diffusion anisotropy maps (a) of a representative boxer (27 yo) and (b) a control (29 yo). Intensity is proportional to anisotropy and color shows the direction. Boxer has decreased FA in genu CC, anterior and posterior limb of IC than those of the normal control. Fiber tracking showed overall less trackable white matter fibers in this boxer’s brain (c) when compared to control (d). The difference in fibers through the corpus callosum is particularly striking.
DTI in Boxing Zhang et al. (2006) 49 professional boxers and 19 controls 42 boxers had normal conventional MRI 7 boxers had NSWM changes None of the boxers exhibited neurological signs or symptoms Boxers had decreased FA in the CC and IC
FA splenium FA genu FA post. FA ant. BDav of CC of CC limb of IC limb of IC (10-5cm2/s)
DTI and ATBI • Cubon et al 2011 • Assessed WM fiber tract integrity 10 varsity college athletes and controls • Also included moderate and severe TBI patients and controls • Symptomatic 1 month after sports-related concussion
DTI and ATBI • Cubon et al. 2011 (cont’d) • Increased mean diffusivity (MD) among athletes c/w controls in several WM tracts in the left hemisphere • Inferior/superior longitudinal fasciculus • Fronto-occipital fasciculi • Retrolenticular part of internal capsule • Posterior thalamic and acoustic radiations
DTI and ATBI • Cubon et al. 2011 • No difference in fractional anistropy (FA) between athletes and controls • FA decreased with the level of severity • MD may be more sensitive in detecting mild injury and FA more sensitive in detecting more severe injury
fMRI and TBI • Jantzen et al. (2004) • Prospective investigation of 8 collegiate football players had preseason fMRI scans obtained during a finger sequencing task • 4 players experienced a concussion during the season and had a f/u fMRI within 1 week of the injury and the 4 controls had a /f/u at the end of the season • Concussed players had marked increased activation in the areas of the parietal, lateral frontal and cerebellar regions
Brain Metabolism is Related to Recovery • Over 200 High School Athletes Studied using fMRI • Tested w/in 7 days of concussion and at point of clinical recovery • Hyperactivation predicts CLINICAL recovery time • Resolution of hyperactivation correlates with recovery on ImPACT Lovell et al., Neurosurgery, 2007
SPECT • Referred population of 17 professional boxers • 14 (82%) had abnormal SPECT scans • 7 cases with frontal lobe hypoperfusion • 3 cases with temporal lobe hypoperfusion • 1 case temporoparietal hypoperfusion • 1 case with frontoparietal hypoperfusion • 1 case with diffuse diminished perfusion in an irregular and patchy distribution • 1 case bilateral cortical thinning
PET • 19 boxers c/w 8 normal controls SPM analysis • 8 hypometabolic areas • Bilateral posterior parietal lobes that extended to the lateral occipital lobes • Bilateral frontal lobes • Bilateral cerebellar hemispheres • Posterior cingulate cortex
Decreased Glucose Uptake Among Boxers (SPM and ROI) Posterior cingulate Bilateral parietal-occipital cortices Bilateral frontal cortices (Broca’s area) Cerebellum
PET/SPECT IN MTBI • Umilie et al. 2002 • 20 patients with MTBI and persistent PCS underwent neuropsychological testing and PET or SPECT • 19 (95%) had neurobehavioral deficits • 18 (90%) had abnormal dynamic imaging on PET or SPECT
PET/SPECT IN MTBI • Umile et al (2002) (cont’d) • 75% - temporal lobe abnormalities • 30% - frontal lobe abnormalities • 40% - nonfrontotemporal abnormalities • Correlations between neuropsychological testing could be established but not consistently • Postulated that there was a temporal lobe vulnerability to TBI
Magnetic Resonance Spectroscopy • Provides in vivo neurochemical information • Metabolites • N-aceytlaspartate (NAA): neuron specific metabolite and is a marker on neuronal health • Choline (Cho): marker of inflammation • Creatine (Cr): stable brain metabolite and a marker of cellular energy status • Myo-inositol: glial marker • Lactate: indirect indicator of ischemia/hypoxia • Can detect areas of neuronal dysfunction in the absence of detectable structural injury
Magnetic Resonance Spectroscopy • Vagnozzi et al. 2008 • Compared 14 concussed athletes (4 boxers) with 5 controls • 3 days after concussion observed a decrease in the NAA/Cr ratio that resolved after 30 days • Concluded that concussion opens a temporal window of metabolic imbalance
Magnetic Resonance Spectroscopy Henry et al. 2009 Compared 12 concussed athletes with 12 non-concussed athletes 24-36 hrs post concussion Concussed athletes had more symptoms Concussed athletes had decreased NAA in the prefrontal and motor cortices
Near Infrared Spectroscopy (NIRS) Non-invasive technique for evaluating cerebral blood volume and oxygenation Technology is based on the transmission and absorption of near-infrared light as it passes through tissue Role in the diagnosis of concussion has been limited May be more useful in the identification of intracranial hematomas
NIRS • Leon-Carrion et al 2010 • Used an infrascanner NIRS device to calculate optical density in brain regions • 35 TBI patients admitted into Neuro ICU • Detected • 90% of extra-axial hematomas • 88.9% of intra-axial hematomas • 93% of nonsurgical hematoma (< 25 ml)
NIRS • Cote et al. 2006 • Monitored cerebral hemodynamics during acute exercise following concussion in 14 male university hockey players • Cerebral oxygenation was reduced up to 35% on day 1 following concussion • Blood volume increased immediately following a concussion at rest and during exercise at day 1 and returned to baseline by day 7 • Concluded that there is an increased demand for oxygenated blood following concussion
BIOMARKERS • S100β • Neuron specific enolase (NSE) • Glial fibrillary acidic protein (GFAP) • Tau (cleaved tau, phospho tau, total tau) • Neurofilament light protein (NFL) • Microtubular associated protein 2 (MAP2) • CK-BB • Spectrin breakdown products • β amyloid protein (Aβ) • Apolipoprotein (Apoe) • Myelin basic protein (MBP) • Ubiquitin C-terminal hydrolase L1 (UCH-L1)
S100 β Most extensively studied serum biomarker Variable relationship between S100β and outcome following MTBI Needs to collected within 4 hours of injury There are extracranial sources of S100β
S100 β • Hasselbatt et al 2004 • 18 marathon runners without brain injury • Found an increase in postrace serum S100β from extracranial sources • No significant change in GFAP
Biomarkers of ATBI in Boxing • Zetterberg et al. (2006) • 14 amateur boxers and 10 healthy controls • CSF analysis 7-10 days and 3 months post bout • Neurofilament light protein (NFL) • Total tau (T-tau) • Phosphorylated tau (P-tau) • Glial fibrillary acidic protein (GFAP) • β amyloid protien (Aβ) • Assessed the number and severity of the hits by interview
Biomarkers of ATBI in Boxing • Zetterberg et al. (2006) (cont’d) • Increases in NFL, T-tau, and GFAP post bout compared to levels post 3 months of rest • NFL and GFAP were higher in boxers post bout compared to controls • No difference in biomarkers between boxers at 3 months and controls except for NFL (remained elevated) • P-tau and Aβ were not elevated • Concluded that amateur boxing was associated with neuronal and astroglial injury
Balance and Agility Testing Balance Error Scoring system (BESS) Sensory Organization Test (SOT) Gait Testing Virtual Reality Instrumented Agility Task
Balance Error Scoring System • Hands lifted off iliac crest • Opening eyes • Step, stumble or fall • Moving hip more than 30 degrees of flexion or abduction • Lifting forefoot or heel • Remaining out of testing position for more than 5 seconds
Balance Error Scoring System Several studies have identified BESS deficits ranging from 3-5 days post concussion when compared to baseline and controls The best sensitivity is at the time of injury
Sensory Organization Test (SOT) Technical force plate system to assess balance Disrupts sensory selection process by altering information from the somatosensory and/or visual inputs while measuring ability to maintain stance Uses 6 different conditions
Sensory Organization Test (SOT) SOT appears to be a sensitive in detecting balance deficits following concussion Limited use on the field secondary to size and technology needs May provide a more technical or refined measure of balance performance BESS is rapid, easy to administer and inexpensive
Postural Stability • Guskiewicz et al. (2001) • 36 concussed athletes compared with 36 matched controls • Assessed postural stability using the SOT and BESS along with neuropsychological testing • Injured subjects demonstrated postural stability deficits on both SOT and BESS
Postural Stability • Guskiewicz et al. (2001) • These deficits were significantly worse than preseason scores and scores of the matched controls on postinjury day 1
Gait Analysis Parker et al 2007 Assessed 29 concussed athletes and 29 uninjured matched controls Gait was assessed while completing a simple mental task At 28 days noted a statistically significant difference in gait stability between concussed athletes compared to controls
Virtual Reality • Slobounov et al 2006 • Assessed balance deficits induced by visual field motion using a virtual reality environment • 8 concussed athletes exhibited balance deficits up to 30 days despite having symptoms and neuropsych testing return to baseline