Download
1 / 88
880 likes | 990 Views
Concussion in the ED What You Know, Need to Know and Better Know to make Correct Treatment. Dave Milzman, MD FACEP Professor of Emergency Medicine Senior Advisor for Clinical Research Georgetown U School Of Medicine Professor of Biology Georgetown University

E N D
Concussion in the EDWhat You Know, Need to Know and Better Know to make Correct Treatment Dave Milzman, MD FACEP Professor of Emergency Medicine Senior Advisor for Clinical Research Georgetown U School Of Medicine Professor of Biology Georgetown University Research Director: Georgetown/WHC EM Residency Clinical Director MedStar Emergency and Trauma Concussion Program Wash, DC
ConcussionDiagnosis , Treatment and Follow Up • Definition: Mild Traumatic Head Injury + LOC with any of 22 common symptoms most common Headache, Dizzy, Fogginess, Trouble Concentrating, Trouble Sleeping • Initial Evaluation: Good Neuro Eval, include Balance Testing, (BESS) and Don’t Image Unless you Plan to Need Admit ( < 0.3% Positive Scan in all Sport Concussion) • Most Important Thing You Can Do On Discharge: • Diagnosis, REST for 3 days, No School, No Sport and Be Re-Evaluated, 60% will Improve in 7 days. • Neuro-Psychology is your Best Consultant !!
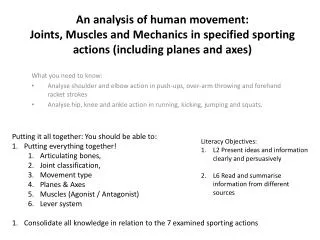
16 year old male • Injury - Elbowed In Forehead During Hockey Game • Initially, No Symptoms, Returned to Ice for 1 shift, But Within 10 Minutes, Became “Foggy” With Poor Concentration, Memory, Dizziness • Subsequent Loss Of Memory For Event, Irritability, Headaches, Reduced Energy, Sensitive To Light And Noise, Sleeping More Than Usual, Poor Balance
Initial Eval, RX and TX • 10th grade honors student • Seen in the ED and sent Home for 1 week no school, lots of sleep , Motrin and Fluids • No texting no gaming, light TV and reading • Concussion Clinic at Day 7 & 14 • Neuropsychological Concussion Evaluation initially demonstrated: • Poor attention • Poor “working memory” • Slowed processing speed • Reduced reaction time • By 14 days, excellent recovery & return to “baseline” values
What Works in Student Athletes • Educate and guide the family and patient and the primary care doctor • Make recommendations for initial accommodations in school • Kept him safe by managing his gradual return to School and Sports • The Easy Decision and return is Sport • Return to Learn is NOT Automatic, • Know This , Practice This ; If Nothing Else, Give all 3 Day Total Rest.
Epidemiology - Concussion • Most frequent diagnosis in injured child is: HEAD INJURY TBI • Every 11 minutes 1 child in the US has a brain injury resulting in permanent disabilities or 35,000 annually • 5,000,000 children with head injuries • 3.8 million concussions/annually Emergency Department Visits • ~ 90%: mild TBI/ GCS 14-15 • Majority with mTBI sent home from ED
STATISTICS • Incidence in HS football = 6%-8% per year. • Boy’s + Girl’s soccer = football. • Girl’s basketball 250% greater risk than Boy’s • Sports and recreational injuries with LOC = 300,000 per year. • Sports and recreational injuries with and without LOC = 1.6 million per year.
DEFINITION Complex pathophysiologic process affecting the brain, induced by traumatic biomechanical forces.
COMMON FEATURES • Caused by a direct or indirect blow to the head, face or neck. • Results in rapid onset of short-lived impairment of neurological function. • A concussion may or may not involve LOC. • The clinical symptoms reflect a functional rather than a structural disturbance.
PATHOPHYSIOLOGY • Mechanism of Injury • Rotational Much Worse than Linear • Impact deceleration • Chemical/Vascular • 1st 7-10 days • ↑K / ↑Ca / ↑glc / ↑glut • ↓CBF • “Period of vulnerability”
Anatomical Timeline of a ConcussionDefining the Key Factors C. Risk Factors A. Injury Characteristics B. Symptom Assessment CONCUSSION Retro- grade Amnesia 20-35% Antero- grade Amnesia 25-40% LOC <10% Neurocog dysfx & Post-Concuss Sx’s Pre-Injury Risks Sec-Hrs Sec-Hrs Hours - Days - Weeks+ Sec-Min
Clinical ProtocolNeurocognitive Testing Pre-Concussion Baseline Testing 1-3 Days Day 5-10 Day 12-16 Concussion *Barth et al., 2002
Pre-Concussion Baseline Testing Concussion Symptoms Cognitive Functions
NEUROCOGNITIVE COMPUTERIZED TESTING • ImPACT (UPMC) • CogSport (Australia) • CRI (Headminder) • ANAM (NRH)
OVERVIEW OF ImPACT • Proven in measures of reliability and validity • Provides useful concussion screening and management information • Validated with multiple peer-reviewed studies • Does not substitute for medical evaluation and treatment • Does not substitute for comprehensive neuropsychological testing
8 separate tests Word memory Design memory X’s and O’s Symbol Match Color Match Three Letters Interference tests 6 composite scores Verbal memory Visual memory Visual motor speed Reaction time Impulsivity Total symptom score IMMEDIATE POST-CONCUSSION ASSESSMENT and COGNITIVE TESTING (ImPACT)
COMPUTERIZED TESTING • Format allows portability and efficiency. • Each vendor has their unique menu of cognitive domains that their product measures. • 20 – 30 minutes to administer. • Used as a “tool” to measure recovery and not to make a diagnosis or solely direct management.
CONCUSSION SYMPTOM SCALE • Standardized survey with 0-6 scale rating • Developed by Lovell and Collins in 1998 • Sensitive tool to measure recovery • Symptoms generally classified into 3 main categories: Physical, Cognitive, and Emotional/Behavioral
Physical Headache Fatigue Dizziness Sensitivity to light and/or noise Nausea Balance problems Emotional Irritability Sadness Feeling more emotional Nervousness 4 Symptom Categories • Sleep • Drowsiness • Sleeping less than usual • Sleeping more than usual • Trouble falling asleep • Cognitive • Difficulty remembering • Difficulty concentrating • Feeling slowed down • Feeling mentally foggy
GENERALMANAGEMENT • Majority of injuries will recover spontaneously. • Physical and cognitive rest are required while symptomatic. • When symptom free and improved “functionally” graduated return to play protocol should be utilized. • Same day return to play—NEVER!!!
PREDICTING RECOVERY TIMELINES ALL ATHLETES ARE NOT CREATED EQUALLY
CONCUSSIONMODIFIERS • Threshold—Repeated concussions occurring with less force or slower recovery. • Age—Child and adolescent < 18 years old. • Co-morbidities—Migraine, depression or other mental health disorders, ADHD, learning disabilities and sleep disorders. • Medication—Psychoactive drugs and anticoagulants. • Behavior—Style of play. • Sport—Contact or collision sport, high-risk.
RETURN TO PLAY PROTOCOL • No activity while symptomatic. • Light aerobic exercise. • Sport-specific exercise—no head impact drills. • Non-contact training drills. • Full contact practice. • Return to game play.
Recovery From Concussion:How Long Does it Take? WEEK 5 WEEK 4 WEEK 1 WEEK 3 WEEK 2 N=134 High School athletes Collins et al., 2006, Neurosurgery
Clinicians’ Return to Play Decisions 100 80 ATC used GSC, SAC, BESS (testing w/ symptom report) 60 40 ATC used only GSC (player symptom report) 20 00 Marshall, Guskiewicz, & McCrea; In Review, 2006.
NFL CONCUSSIONGUIDELINES • Established in 2009. • No same day return to practice or game play. • Players encouraged to be honest and report symptoms. • Independent neurology opinion for each injury.
CHRONIC TRAUMATIC ENCEPHALOPTHY • NFL Survey— • > 50 = 5x risk • 30-49 = 19x risk • Comparative data from the Framingham heart study. • Concept of subconcussive trauma. • Sports Legacy Institute.
Concussion’s Effects on School Learning & Performance “Which specific types of problems are you experiencing in school?” Students reported an average of 4 problems below. Headaches interfering 71.3% Can’t pay attn in class 62.5% HW taking much longer 59.5% Difficulty studying for test/quiz 51.9% Too tired 50.6% Diffic understanding material 44.0% Difficulty taking notes 28.8%
Concussion’s Effects on School Learning & Performance “Which classes are you having the most trouble with?” (Percent reporting trouble in class) Parent Student Math 60.3% 73.7% Reading/LA 38.1% 46.1% Science 38.1% 47.4% Soc Stud 38.1% 40.8% Foreign Lang 38.1% 38.2% Music 6.3% 17.9% PE 7.9% 10.5% Art 3.2% 5.3% -None 25.4% 6.6%
General Principles of Recovery No additional forces to head/ brain Resting the brain & getting good sleep Managing/ facilitating physiological recovery Avoid activities that produce symptoms Not over-exerting body or brain Ways to over-exert Physical Cognitive! (concentration, learning, memory) (Emotional) Even taking Neuro-Cognitive Testing is Contra-Indicated in Symptomatic Patient
Consensus Statement on Concussion in Sport 4th International Conference on Concussion in Sport held in Zurich, November 2012
Zurich CIS Consensus • Concussion Management • Physical AND Cognitive Rest 48-72 Hours • Graduated RTP: when asymptomatic at rest • stepwise progression, proceed to next level if asymptomatic at current. • Each step take 24 hours; would take approximately one week to proceed through the full rehabilitation protocol • Same Day RTP: NEVER appropriate in child or adolescent student-athlete (possible in adult ONLY if within well established system) • Recognized delayed onset of symptoms 15-30 minutes is Usual
Changing Presentation Rates For mTBI (Concussion) And Changing Imaging Rates. Dave Milzman, MD, FACEP Sam Frankel MS, Colin Leiu MS, Katy Taxiera, Steve Swinford MS, Zach Hatoum. Georgetown U. School of Medicine, Wash D.C. MedStar Sport Concussion Center; Wash, D.C.
2000-2012: Rapid rise in past 5 year with number of concussions increased by 140% compared to ED and Trauma patient volume increased only by 23.9%; p< 0.02. • Increases in CT for concussion: 25.8% /10 yr with less than 1.2% of mTBI with positive Head CT ; 24% MRI have No- Therapeutic Positive Findings MEANING • None Required NeuroSurgical Intervention. Results
Discussion Media And Medicine Has Met And Increased Awareness As mTBI Presentation And Concussion Visits are Increasing at Increased rates Compared to All other ED and Trauma Visits CT and MRI Increased In Use With No Improved Treatment Intervention.
Controversy over CT for Minor TBI Arguments for liberal use of CT: • Preventable morbidity/mortality due to unrecognized TBIs • CT provides visual information about the skull and the brain • Preverbal children difficult eval. • When indicated, benefit of CT greatly outweighs risk, however…
Investigations • Neuroimaging (CT, MRI) • Contributes little to concussion evaluation • Use when suspicion of intracerebral structural lesion exists: • prolonged loss of consciousness • focal neurologic deficit • worsening symptoms • Deterioration in conscious state • MRI still not proven benefit aids detection not treatment.
Controversy over CT for Minor BHT Arguments against liberal use of CT: • Of the 325,000 children evaluated with CT after BHT, fewer than 1% have significant TBI and < 0.3% require any Neurosurgical intervention. • Drawbacks of CT include transport outside the ED, pharmacological sedation, costs (charges $2-3K/patient) • lethal malignancy risk from CT may be as high as 1:1250
Lifetime Cancer Mortality Risk NEJM, Brenner et al. • Lifetime cancer mortality risk with single CT head in year 1 of life: • i-V
PECARN Prediction Rules Age 2 years and older GCS < 15 or abnormal mental status LOC History of emesis Severe mechanism of injury Signs of basilar skull fracture Severe headache Kuppermann/Holmes/Dayan/Hoyle/Atabaki et al 2009
Results—Positive CT Proportion* * Preliminary data. O.R. = 3.01 (95% CI 2.07-4.37)
Traumatic Brain Injury Glasgow Coma Scale “Minimal” Mod Severe Mild ? Severe GCS ≤ 8 Moderate GCS 9 - 12 Mild GCS 13 - 15 Teasdale et al Lancet 1974; Sports concussion