Download
1 / 30
370 likes | 1.1k Views
ACQUIRED HEMOSTATIC DISORDERS. Lugyanti Sukrisman Div. of Hematology & Medical Oncology Dept. of Internal Medicine University of Indonesia/ Cipto Mangunkusumo Hospital. BLEEDING Liver diseases ITP Acquired qualitative platelet defects Def of vit K-dependent factors

E N D
ACQUIRED HEMOSTATIC DISORDERS LugyantiSukrisman Div. of Hematology & Medical Oncology Dept. of Internal Medicine University of Indonesia/ CiptoMangunkusumo Hospital
BLEEDING • Liver diseases • ITP • Acquired qualitative platelet defects • Def of vit K-dependent factors • Excessive fibrinolysis THROMBOSIS • Disseminated intravascular coagulation • Antiphospholipid syndrome • Pathologic anticoagulant • (immune coagulopathies) ACQUIRED HEMOSTASTIC DISORDERS
Liver’s central role in hemostasis: • The major site of synthesis of • all coagulation factors (except vWF), • regulatory proteins of coagulation system (antithrombin, protein C & S), • component of fibrinolytic system • Clearance of activated clotting factors from circulation A. Coagulation abnormalities of liver diseases (1) Colman RW. Hemostasis & thrombosis. Basic principles & clinical practice 2006
Thrombocytopenia • Platelet dysfunction • Coagulation abnormalities • Disseminated intravascular coagulation & hyperfibrinolysis A. Coagulation abnormalities of liver diseases (2) Colman RW. Hemostasis & thrombosis. Basic principles & clinical practice 2006
Pathogenesis: • Splenic sequestration due to portal hypertension • Impaired platelet production • Thrombin-mediated platelet consumption • HCV infection: • Viral infection of megakaryocytes • Platelet destruction due to autoimmune mechanisms 1. Thrombocytopenia
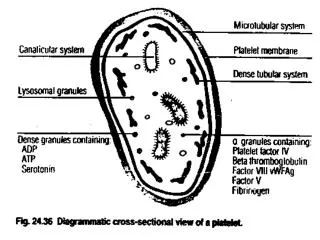
Reduced platelet adhesion • Impaired platelet aggregation 2. Platelet dysfunction Colman RW. Hemostasis & thrombosis. Basic principles & clinical practice 2006
Reduced of vit-K-dependent coagulation factors (II, VII, IX, X) & F. V • Fibrinogen: normal/increased decreased: • Impaired synthesis • Increased catabolism • Loss into extra vascular space • Massive hemorrhage • Diminished antithrombin, protein C & S, heparin cofactor II, α-2 macroglobulin 3. Coagulation abnormalities Colman RW. Hemostasis & thrombosis. Basic principles & clinical practice 2006
History of jaundice/acute hepatitis, risk of infection (iv drug user, liver disease in family, etc) • (History of) bleeding: hematemesis &/melena • Clinical sign of liver disease & complication: • Jaundice • Other signs: pale, ascites, splenomegaly, palmarerythema, edema, etc • Bleeding signs: petechiae, hematoma, hematemesis/melena, etc Diagnosis (1)
Laboratory results: • CBC: thrombocytopenia ± anemia/leukopenia • Liver function tests: low albumin level, increased transaminase/bilirubin (variably) • Coagulation tests: PT, aPTT, fibrinogen, D-dimer • Hepatitis markers (hepatitis B/C) • Abdominal US: liver disease & others (bile stone, etc) • Others: endoscopy of upper GI Diagnosis (2)
Active bleeding/plan of invasive procedure: • Vit K, FFP/cryoprecipitate, platelet concentrate, packed red cells • Stop the bleeding: ligation/sclerosing therapy & pharmacology treatment • Treatment of liver disease & complication, non pharmacologic treatment & nutritional support Treatment
Consumptive coagulation • Defibrin(ogen)ation syndrome • Thrombohemorrhagic syndrome B. Disseminated intravascular coagulation
Marder VJ. Hemost and Thromb.. 2006.1571-1600 Activation of coagulation Events leading to bleeding Events leading to thrombosis Circulating thrombi Circulating fibrin degradation products Consumption of platelets and coagulation proteins Thrombotic occlusion of microcirculation of all organs Fibrinolysis in microcirculation + • Signs of microvascular thrombosis • Neurologic : multifocal, delirium, coma • Skin : focal ischemia, superficial gangrene • Renal : oliguria, azotemia, cortical necrosis • Pulmonary: acute respiratory distress • syndrome • GI: acute ulceration • Fragmentation hemolytic anemia • Signs of hemorrhagic diathesis • Neurologic : intracerebral • bleeding • Skin : petechiae, ecchymoses, • venipunctureoozing • Renal : hematuria • Mucous membranes: epistaxis, • gingival oozing • GI: massive bleeding Marder VJ. Hemost and Thromb. 5edt. 2006.1571-1600
Underlying disorder Systemic activation of coagulation Consumption of platelets and clotting factors Widespread intravascular fibrin deposition (severe) Bleeding Thrombosis and organ failure
Complexity and variability depends on: • Triggering event(s) • Host Response • Comorbid conditions Clinical manifestation
Clinical features Bleeding: mucosal oozing, ecchymoses, petechiae, massive GI blood loss Renal/cerebral/ hepatic dysfunction, ARDS • Laboratory • Increased D-Dimer level • Increased FDP level • Decreased AT level • Decreased platelet level • Bload smear:schistocytes • Decreased fibrinogen level • Prolonged thrombin time/aPTT/PT Diagnostic approach
Severe liver failure/liver disease • Vitamin K deficiency • HELLP syndrome • Thrombotic thrombocytopenic purpura • Congenital abnormalities of fibrinogen Differential Diagnosis
Treat the underlying disease • Restore the circulation • Replacement therapy • FFP/cryoprecipitate, platelet concentrate, packed red cells • Other pharmacologic therapy: • Heparin, antithrombin, activated Protein C, others TREATMENT OF DIC
vitamin K: essential for the final postribosomal carboxylation of coagulation factors II, VII, IX, X and protein C and protein S • laboratory features: prolonged PT &decreased factors II, VII, IX, X level • in severe, protracted vitamin K deficiency: prolonged aPTT C. Deficiency ofvitamin K-dependent factors
I. Inadequate supply: 1. Dietary deficiency 2. Destroying the gut flora by administration of broad-spectrum antibiotics II. Impaired absorption of vitamin K: 1. Biliary obstruction (gallstone, tumor) 2. Malabsorption of vitamin K 3. Drugs (cholestyramine) III. Pharmacologic antagonists of vitamin K (coumarins, warfarin) Vitamin K deficiency
D. Excessive fibrinolysis • Primary fibrinolysis (excessive release of tissue Plasminogen Activator): rare • Acquired: • Thrombolytic therapy • Secondary disease-related: • surgical/ trauma • neoplasms (prostate, pancreas, leukemia) • systemic lupus erythemathosus • severe liver disease (defective clearance of activator) • Fibrinolysis secondary to intravascular coagulation Ratnoff OD, Forbes CD. Disorders of hemostasis 1996, 296-322
Diagnosis • Bleeding signs • Thrombolytic therapy/other condition related to acquired excessive fibrinolysis • Laboratory: • FDP: increased • Plasma fibrinogen level: reduced • Euglobulin clot lysis time: rapid • TT, PT, aPTT: prolonged Ratnoff OD, Forbes CD. Disorders of hemostasis 1996, 296-322
Treatment of excessive fibrinolysis • Fibrinolytic inhibitors: • Tranexamic acid • -Aminocaproic acid (EACA) • Fibrinolytic inhibitor: contraindicated for fibrinolysis secondary to/associated with intravascular clotting Ratnoff OD, Forbes CD. Disorders of hemostasis 1996, 296-322
E. Pathologic anticoagulants (immune coagulopathies) (1) • Appear spontaneously in subjects with previously normal hemostatic function. • Antibodies to factor VIII, “idiopathic” inhibitor • Autoimmune disorders (SLE, rheumatoid arthritis, multiple sclerosis, pemphigus, etc) • Hematologic malignancies: chronic lymphocytic leukemia, non-Hodgkin lymphoma, multiple myeloma, etc • Drug reactions: allergies to penicillin, sulfonamides, chloramphenicol, methyldopa, etc
E. Pathologic anticoagulants (immune coagulopathies) – (2) • Prolonged aPTT • Reduced F. VIII levels • Inhibitor F. VIII • Spontaneous, often severe/life-threatening bleeding Colman RW. Hemostasis & thrombosis. Basic principles & clinical practice 2006