Download
1 / 48
741 likes | 2.71k Views
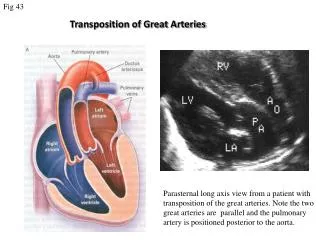
Corrected Transposition of Great Arteries. Seoul National University Hospital Department of Thoracic & Cardiovascular Surgery. Congenitally Corrected Transposition of Great Arteries. Introduction 1. Definition A cardiac anomaly with ventriculo-arterial discordant connection

E N D
Corrected Transposition of Great Arteries Seoul National University Hospital Department of Thoracic & Cardiovascular Surgery
Congenitally Corrected Transposition of Great Arteries • Introduction • 1. Definition • A cardiac anomaly with ventriculo-arterial discordant connection • (transposition of great arteries) & atrio-ventricular discordant • connection (right atrium connecting to left ventricle & left atrium • to the right ventricle). • The circulatory pathways are therefore in series. • 2. History • Rokitansky : 1st description in 1875 • Schiebler : Clinical syndrome in 1961 • Anderson, Lillehei : 1st repair in 1957 • Ilbawi et al : Double switch operation in 1990
Congenitally Corrected TGA • Pathophysiology • Combined AV & ventriculo-arterial discordance resulting in corrected transposition of systemic and pulmonary circulations. • There is high incidence of associated intracardiac anomalies including VSD, pulmonary outflow tract obstruction, tricuspid insufficiency, and AV conduction anomalies.
Ventriculo-arterial Discordance • Morphologic characteristics • Diagrammatic models of four basic hearts
Congenitally Corrected TGA • Surgical morphology • 1. Ventricle (conus, loop, position) • Dextrocardia • 2. Pulmonary outflow tract; • Transverse plane & wedged • 3. Atrial, ventricular septal position • 4. Tricuspid, mitral, aortic valves • 5. Ventricular septal defect • 6. Atrioventricular node & bundle of His • 7. Coronary arterial patterns • 8. Associated anomalies • no coexistent cardiac anomalies in 1 ~ 2 %
Congenitally Corrected TGA • Associated cardiac anomalies • Ventricular septal defect : 86% • Pulmonary stenosis : 64% • Tricuspid regurgitation : 28% • AV block : 12%
Surgical morphology Congenitally Corrected TGA
Congenitally Corrected TGA Surgical morphology
Congenitally Corrected TGA Surgical pathology Morphologic LV
Congenitally Corrected TGA Surgical pathology Morphologic RV
Congenitally Corrected TGA Surgical pathology Morphologic RV VSD Morphologic LV
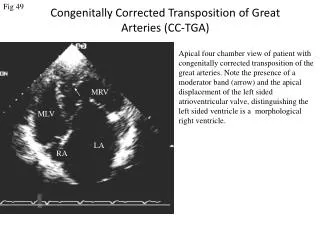
Congenitally Corrected TGA • Clinical features & diagnosis • 1. Pathophysiology • * Determined by VSD & pulmonary stenosis ; usually mild symptom, • not severe pulmonary stenosis in infancy • * Most often, presentation is in childhood or in second decade ; • growth failure, exercise intolerance, cyanosis • * Left sided tricuspid valve incompetence seems to worsen with time • * Bradycardia, WPW syndrome • 2. Physical findings • Not diagnostic • 3. Additional investigations • 1) Chest radiography : ascending aorta along left upper cardiac silhouette • 2) EKG • 3) Echocardiography • 4) Cardiac catheterization & cineangiography
Congenitally Corrected TGA • Natural history • 1. Incidence • 0.5% - 1.4% of CHD, slightly male predominating • 2. Heart block • 1) Complete heart block • 5 - 10% at birth, 10 - 15% in adolescence, 30% in adult • 2) 1st or 2nd degree A-V block ; 40 - 50% at birth • 3) 40% retain normal PR interval & QRS through their lives • 3. Ventricular function • Not truly normal, but sufficiently good in most & tendency • to deteriorate after 2nd decade of life • 4. Effect of coexisting cardiac anomalies • VSD, PS, left-sided A-V valve incompetence
Congenitally Corrected TGA • Operative Indications of cc-TGAConventional Repair • The presence of corrected TGA is not an • indication for a reparative operation. • 1. Ventricular septal defect • * same as normal heart • 2. VSD & important PS • * same as TOF • 3. Left-sided tricuspid incompetence • * same as mitral incompetence • 4. Complete heart block
Congenitally Corrected TGA • Operative techniques • 1. Repair of ventricular septal defect • 2. Repair of coexisting VSD & PS • * Extracardiac conduit • * Without extracardiac conduit • * One & a half ventricle repair • 3. Correction of incompetent tricuspid valve • * Repair (annuloplasty) • * Replacement • 4. Fontan-type repair • Straddling, A-V canal , & hypoplastic ventricle • 5. Anatomic correction (double switch operation)
Congenitally Corrected TGA Morphologic characteristics
Surgical view Congenitally Corrected TGA • Rt. sided AV valve through Rt. atriotomy
Congenitally Corrected TGA • Surgical view • Rt. sided AV valve & ASD through Rt. atriotomy
Congenitally Corrected TGA • Surgical view • VSD through Rt. sided atrioventricular valve
Congenitally Corrected TGA Repair of VSD
Congenitally Corrected TGA Apico-pulmonary artery conduit
Congenitally Corrected TGA Repair of VSD + PS Standard repair of situs solitus congenitally corrected TGA, VSD, and PS
Congenitally Corrected TGA One & a half ventricle repaircc-TGA, VSD, PS VSD closure, pulmonary valvotomy, and inparallel BCPC
Congenitally Corrected TGA Double switch operation • Bidirectional superior cavopulmonary anastomosis and • hemi-Mustard modification for double switch procedure
Congenitally Corrected TGA Double switch operation • Senning plus arterial switch operation
Congenitally Corrected TGA • BCPC in anatomic correction • It may benefit the small or poorly functioning RV • It importantly reduces complexcity of the atrial baffle procedure • It eliminates complications related to the superior limb of the atrial baffle • It reduces flow across an RV-pulmonary trunk conduit • It likely increases conduit longevity
Congenitally Corrected TGA • Anatomic correction • The evidence is strong that right ventricle should not remain in the systemic circulation as it does after a conventional repair • A combined arterial switch and Senning operation ( double switch operation ) is an option for patients with cc-TGA with two ventricles of adequate size for biventricular repair and a normal pulmonary valve • The timing of surgery is difficult to choose because this is a long and complex operation of Rastelli and atrial switch procedure in patients with cc-TDA & VSD , & PS or atresia
Congenitally Corrected TGA • Results of conventional repair • 1. Survival • * Early deaths • * Time-related survival • 2. Modes of death 3. Incremental risk factors for death • * Abnormalities of conduction system • * Abnormalities of ventricular function • * Regurgitation of systemic tricuspid valve • 4. Post-repair complete heart block • 5. Left-sided tricuspid valve incompetence • 6. Ventricular function & functional status
Congenitally Corrected TGA • Problems of physiologic repair • Progressive tricuspid regurgitation • Right ventricular dysfunction • Atrioventricular dysfunction • Conduit related problems
Congenitally Corrected TGA • Tricuspid regurgitation • Volume load on the right ventricle • Low incidence with naturally occurring pulmonary stenosis • Movement of interventricular septum
Congenitally Corrected TGA • Tricuspid valve abnormality • In IVS Preop. 38% postop. 60% • In VSD Preop. 90% postop. 56% • In VSD+PS Preop. 36% postop. 36%
Congenitally Corrected TGA • Causes of Tricuspid Regurgitation • Structural alteration of tricuspid valve component Congenitally abnormal tricuspid valve Adherence of septal leaflet or chordae to VSD patch Asynchronous papillary muscle contraction with RBBB Supraventricular or ventricular arrhythmia • Abnormal function of structurally normal valve Dilated annulus Distraction of papillary muscles Right ventricular or papillary muscle dysfunction
Atrioventricular Discordant Connection • Introduction • Definition A congenital anomaly in which right atrium connects to left ventricle (LV) and left atrium connects to right ventricle (RV). • History Ruttenberg ; AV discordant with DORV in 1964 Brandt ; AV discordant with DOLV in 1966 Van Praagh ; Isolated ventricular inversion in 1966 Isolated atrial inversion in 1972 Brandt ; Surgery for AV discordant with DOLV in 1966
AV Discordant Connection • Morphology • Ventricular architecture • Ventricular position & rotation Positional anomalies ; superior-inferior ventricles Rotational anomalies ; criss-cross pathway • Ventricular size • Cardiac position • Ventriculoarterial connection • AV node & bundle of His • Accessory conduction pathways • Coronary arteries • Atrioventricular valves
Isolated Atrial Inversion • Surgical morphology
Isolated Ventricular Inversion • Surgical morphology • Isolated ventricular inversion (A), & anatomically • corrected malposition of the great arteries (B)
AV Discordant Connection • Clinical features & diagnosis • Clinical features of AV discordant connection vary widely, depending on ventriculo-arterial connection and associated cardiac anomalies • Congenitally corrected TGA VSD, PS • DORV and DOLV VSD, PS • Isolated ventricular or atrial inversion Similar to TGA, PS add additional cyanosis
AV Discordant Connection • Natural history • Most of the information concerning natural history drawn from patients with corrected TGA should be expected, & other morphologic findings may affect natural history • Patients with situs inversus are more likely to have DORV and TOF physiology, but less likely to have systemic AV valve regurgitation and heart block then patients with situs solitus
AV Discordant Connection • Surgicai indications The diagnosis of DORV, DOLV, and isolated ventricular or atrial inversion in patients with AV discordant connection are indications for operation, but each has special considerations. • Technique • Congenitally corrected TGA • DORV+PS • DOLV • Isolated ventricular or atrial inversion • Placing epicardial pacemaker leads
Isolated A-V Discordance • Surgicai procedures • VSD closure The position of the conduction bundle locationwas assumed to be akin to that in congenitally corrected transpositionof the great arteries in the anterosuperior edge of the septaldefect • Senning RepairNative interatrial septum sufficed for the intra-atrial baffleutilized to separate the pulmonary veins from the mitral valvein all four Senning repairs.
AV Discordant Connection • Results of surgical treatment • Survival Early death Time-related survival • Mode of death • Incremental risk factors for death AV discordant connection ; probably major VA discordant connection ; probably not recently • Postrepair heart block • Other outcome events Others as in cc-TGA ( TR, Block, Function, etc) Use of valved conduit
Anatomically Corrected Malposition of Great Arteries • Introduction • Definition Anatomically corrected malposition is an anomaly in the position of the great arteries and not in cardiac connections. The aortic origin lies to the left and usually anterior to the pulmonary trunk origin when there is situs solitus and the circulatory pathways remain in series. • History Theveanin ; 1st report in 1985 Harris & Farber ; Termed anatomically corrected malposition Raghib ; Described isolated bulbar inversion in corrected transposition Van Praagh ; Described in 1967 using the term of anatomically corrected transposition of great arteries
Corrected Malposition of GAs • Morphology • Structure of sinus portions of both ventricle is normal • There are abnormalities of the outlet, or infundibulum, in both ventricle. • The LV probably always exhibits a subaortic conus • The RV may also have an infundibulum, but it may be less well developed and in some case is absent • The aorta lies to the left and usually anterior to the pulmonary trunk
Corrected Malposition of GAs • Associated anomalies • Commonly large VSD, usually conoventricular • Pulmonary stenosis is usual, often infundibular • Subaortic stenosis may occur • Tricuspid atresia or hypoplasia in half & RV hypoplasia
Corrected Malposition of GAs • Clinical features & diagnosis • Clinical features depend on associated anomalies. • Characteristic appearance of L-malposition in chest radiograph • The natural history is affected as typical for the associated cardiac anomalies
Corrected Malposition of GAs • Technique of operation Determined by associated cardiac anomalies, such as Fontan operation in hypoplastic ventricle VSD closure & PS relief when necessary • Indications for operation Anatomically corrected malposition is not an indication for operation. Coexisting cardiac anomalies may present an indication for operation.