Download
1 / 16
270 likes | 1.37k Views
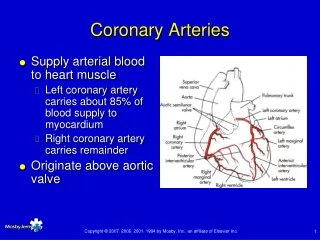
Transposition of Great Arteries ( TGA ) Dr.Aso faeq salih pediatric cardiologist. 5 % of all CHD. Types d – TGA . l – TGA. d – TGA. the aorta is anterior & to the R of pulmonary artery . Survival depends on patency of foramen ovale & Ductus Arteriosus . 1/2 of patients VSD .

E N D
Transposition of Great Arteries(TGA)Dr.Aso faeq salihpediatric cardiologist
5 % of all CHD • Types • d – TGA . • l – TGA .
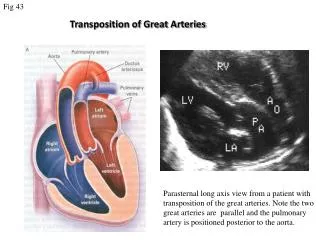
d – TGA • the aorta is anterior & to the R of pulmonary artery . • Survival depends on patency of foramen ovale & Ductus Arteriosus . • 1/2 of patients VSD . • M : F 3 : 1 . • > common CHD in infants of diabetic women . • Before the advent of surgery mortality > 90 % in the first year of life .
Clinical manifestations • Cyanosis & dyspnea within 1st hrs. or days of life . • Hypoxemia is severe , HF is less common . • Signs : • Cyanosis • S2 single & loud . • Murmurs are usually absent unless there is associating lesions
Investigations • CXR : • Mild cardiomegaly , narrow mediastinum , normal or increased pul. Vascularity . • Egg shaped heart . • ECG: normal neonatal R – sided dominant pattern . • Arterial Po2 low & not changed following hyperoxia test with 100% O2 . • Echo & Doppler : confirm the diagnosis . • Cardiac catheterization : palliative tretament
Treatment : • PGE2 infusion to maintain a patent DuctusArteriosus • Cath and Surgery : • Rashkind balloon Atrial Septoplasty . • Arterial switch( Jantene) : treatment of choice , timing 1st 2 weeks , if delayed decrease LV mass . • Mustard operation .
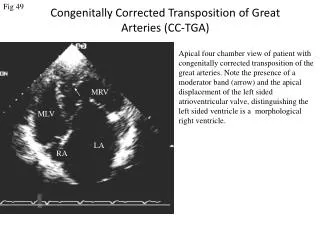
Prognosis : • Depends on patency of Ductus Arteriosus , associating defects ( VSD provide a better mixing of blood ) . • Without surgery death within 1st year of life . l – TGA RA is connected with LV & LA is connected with RV , the great arteries also transposed the circulation is physiologically corrected .
Pulmonary stenosis • Common as PDA,
There are four different types of pulmonary stenosis: valvar pulmonary stenosis - the valve leaflets are thickened and/or narrowed-fusion of valves- leave a small eccentric hole in middle supravalvar pulmonary stenosis - the pulmonary artery just above the pulmonary valve is narrowed
subvalvar (infundibular) pulmonary stenosis - the muscle under the valve area is thickened, narrowing the outflow tract from the right ventricle branch peripheral pulmonic stenosis - the right or left pulmonary artery is narrowed, or both may be narrowed
The following are the most common symptoms of pulmonary stenosis. heavy or rapid breathing shortness of breath Fatigue , fainting rapid heart rate Cyanosis in terminal stages Severe cases: Distended jugular veins, hepatomegaly, ascites
Repair options include the following: 1. balloon dilation or valvuloplasty used for valvar, supravalvar, or branch types of pulmonary stenosis 2. ValvotomyValvotomy is the surgical release of adhesions that are preventing the valve leaflets from opening properly. This type of procedure is generally not performed, as balloon dilation or valvuloplasty has become more common