Download
1 / 16
160 likes | 438 Views
Bowman’s layer. Descemet’s membrane. Pathologic Diagnosis. Diagnosis Pseudophakic bullous keratopathy with Chronic bullous keratopathy Degenerative pannus Stromal edema Severe endothelial atrophy. Pseudophakic bullous keratopathy. Iatrogenic disease

E N D
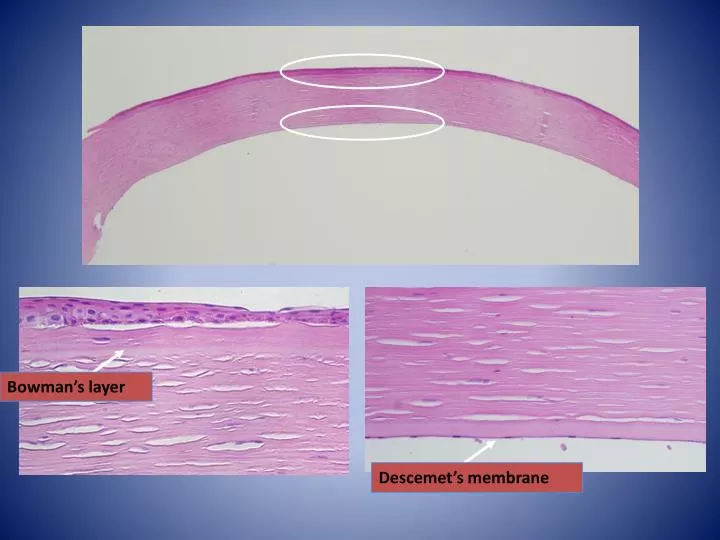
Bowman’s layer Descemet’s membrane
Pathologic Diagnosis • Diagnosis • Pseudophakic bullous keratopathy with • Chronic bullous keratopathy • Degenerative pannus • Stromal edema • Severe endothelial atrophy
Pseudophakic bullous keratopathy • Iatrogenic disease • Direct or delayed endothelial damage associated with cataract surgery and intraocular lens implantation • One of the most common indications for corneal transplantation.
Pseudophakic bullous keratopathy • Histology • Subepithelial bullae • Stromal edema • Severe endothelial loss • Descemet’s membrane is NOT thickened with regular caliber WITHOUT guttate excrescences
PannusFlat superficial scar of the anterior cornea Degenerative pannus Chronic edema and bullous keratopathy Layer of connective tissue between the epithelium and Bowman’s layer (BL) BL remains intact Inflammatory pannus Tracoma Subepithelial ingrowth of inflamed fibrovascular tissue from limbus Destroys BL
Case History • 64 yo M • Gross description ( Contributor ) • Endothelial cells of right eye • 0.5 x 0.3 cm translucent shave
Diagnosis • Fuchs’ endothelial dystrophy
Descemet’s stripping with endothelial keratoplasty (DSEK) • Alternative to corneal transplantation for patients in primary dysfunction of the cornea endothelium. • Advantages over traditional keratoplasy • Minimal refractive change • More rapid visual recovery • Maintenance of the structual integrity of the recipient’s cornea
Fuchs’ dystrophy • Often bilateral –may be asymmetric • Late onset, slow progression • Patient generally present s after age 50 • Female predominance • Autosomal dominant inheritance • Associated with several mutations in the gene for collagen type VIII at 1p34.2-p32
Fuchs’ dystrophy • Histology • Subepithelial bullae • Stromal edema • Atrophy of endothelium • Mulitilaminar thickening of Descemet’s membrane with guttate excrescences in the central cornea • Cytoplasm of the residual endothelial cells contain round granules of melanin pigment from iris pigment epithelium
Case History • 54 yo WF, Irritable, infected right eye for 4 M. • Vision : 20/30 OD, 20 /15 OS. • IOP: 50 mm Hg, OD, 12mm Hg OS. • Fleshy brown mass in the anterior chamber angle inferonasally. • 3mm in width and was accompanied by and ectropion uveae. • Marked cupping of the right optic disc. • Diagnosis at time of enucleation was intraocular tumor with secondary glaucoma.
Case History (Gross) • 25x25x24 mm with 1 mm ON. • Clear cornea :11 x10 mm. • The eye transmitted light well. • Pigment was scattered along the back of the cornea, and AC was deep. • Chamber angle inferiorly was filled with a slightly elevated gray mass.