Download
1 / 51
520 likes | 547 Views
Explore the history, rationale, physiology, and patient selection for intrathecal drug delivery of opiates, highlighting dosing strategies, pump options, and therapeutic evaluation.

E N D
Neuromodulation for Failed Back Surgery SyndromePart II Richard K. Osenbach, M.D. Director of Neuroscience and Neurosurgery Cape Fear Valley Health System Fayetteville, NC
INTRATHECAL DRUG DELIVERY
Spinal Opiates for Benign Pain • Controversial • Mixed reviews and results • Reporting of outcomes non-uniform • No definitive end-point for therapy
Rationale of IT Drug Infusion Provide high concentration of drug at the site of interaction with spinal receptors and minimize spread to other regions in the brain
History of Opiate Analgesia • 1901 - intrathecal injection of morphine • 1915 - antagonist of morphine discovered • 1951 - 1st human use of morphine antagonists • 1976 - 1st use of IT morphine in animals • 1980 - spinal morphine used for cancer pain
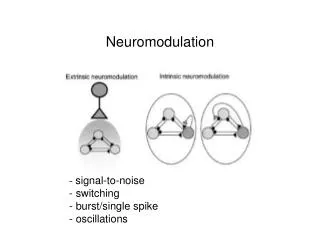
Opioid Receptors and Ligands • Location of Opioid Receptors in the CNS • Dorsal horn • Lamina I • Substantia gelatinosa • Brainstem • Nucleus caudalis • Supraspinal • PAG • Thalamic nuclei • Striatum • Hypothalamus • Limbic system • Cortex
Mu Receptor • Defined by affinity for morphine • Less affinity for other receptor subtypes • Most clinically important opioids selective for Mu receptor • Cross react at higher doses • 1 - supraspinal 2 – spinal • Most analgesic effects of systemic morphine mediated through 1 effects • 70% located pre-synaptically
Opioid Recptor Physiology • G-protein-coupled receptor family • Synthesized in DRG • Second messenger using cAMP • Negative coupling • Inhibit cAMP via Gi-protein • And - opening of K+ channels • - Closing of ca2+
Opioid Actions • Analgesia • Pruritis • Urinary retention • Autonomic Effects • Cough suppression, orthostatic hypotension • Nucleus tractus solitarius and ambiguous, locus ceruleus • Respiratory depression • Nucleus tractus solitarius, parabrachial nucleus • Nausea/vomiting • Area postrema • Constipation • Meiosis • Superior colliculus, pretectal nuclei • Endocrine effects • Posterior pituitary – inhibition of vasopressin • Hormonal effects – hypothalamic infundibulum • Behavioral effects • Amygdala, hippocampus, nucleus accumbuns, basal ganglia • Motor rigidity • Striatum
Intraspinal MorphineConversion Ratios • 300 mg oral morphine = • 100 mg parenteral morphine = • 10 mg epidural morphine = • 1 mg intrathecal morphine * May not be accurate at high doses
Patient Selection • Inclusion Criteria • Opioid-responsive pain • Failure of long-acting oral opioids • Exclusion Criteria • Spinal pathology precluding catheter placement • Allergy to opiates • Difficulty coming for pump refills
Catheter tip Pump anchored with sutures or pouch Dural puncture Paramedian Oblique Entry V-wing anchor Loop of excess catheter under pump 5 cm of slack in catheter Catheter connector which also functions as the primary anchor
Implantable Drug Pumps • Programmable • Constant flow
Constant Flow Pump • Drug delivered at constant, pre-programmed rate • ADVANTAGES • Unlimited life expectancy • Less costly (?) • DISADVANTAGES • Less versatile than programmable pumps • Dose changes require pump refill • Flow rates influenced by physical parameters
Body temperature 10-13% increase in flow per 1ºC rise Geographical elevation flow increases at higher altitudes Blood pressure inversely proportional 3% change for every 10mmHg MAP Drug viscosityQ = K x (P1-P2) u Reservoir capacity flow rate calibrated for 50% capacity;4% variability at extremes of volume Pump “Dead Space” 4ml “dead volume” correction factor for concentration Constant Flow PumpFactors Affecting Drug Delivery
Programmable Pumps ADVANTAGES • Maximum flexibility • Variable rates • Program bolus doses • Alter dose by telemetry DISADVANTAGES • Finite life expectancy • More expensive (?)
General Guidelines for IT Drug Selection Consider these issues regarding administration of intrathecal drugs: • Drug stability • Drug-drug compatibility for co-administration • Drug-pump compatibility • Effect of diluents on pump • pH Choose appropriate concentration based on: • Desired dose • Pump capabilities • Refill interval (no less than 2-4 wks)
General Guidelines (cont.) DOSING STRATEGY • Dose escalation with inadequate analgesia • Cautious dose reduction if adequate analgesia but intolerable side effects • Addition of drug; reduction of opioid dose with second analgesic EVALUATION OF THERAPEUTIC FAILURE • Comprehensive patient reevaluation • Assess pump and system integrity • Interrogate and empty (refill assess volume) – Dye study of catheter integrity • Pathophysiology of the pain
Trialing for IT Therapy What do we know about screening? • Multiple accepted methods • No consensus as to the single best method
Questions Regarding Trialing • Screening method • Duration of trial • Drug and dose • Use of placebo • Systemic opioids • Criteria for success
Functional (Continuous) Trial ADVANTAGES • Most accurately replicates permanent pump • Allows for longer trials • Controlled dose titration • Assess starting dose for IT therapy • Reduce risk of drug-related side effects • Dissipates placebo effect over time • Assessment of functional outcome DISADVANTGES • Procedurally more complicated • Requires greater expertise • Higher morbidity • More costly
Placebo Administration • Rationale: reduce the likelihood of a false positive trial • Normal individuals may exhibit a placebo response • Difficulty interpreting placebo response • A positive placebo response should not necessarily mean “no pump” • Functional trialing with dose titration dissipates the placebo response over time
Oral Opioids During Trial • No consensus on alteration of systemic opioids during the trial • Maintaining the patient on a portion of their daily dose will lessen the likelihood of withdrawal • Withdrawal from systemic opioids may result in reduction in opioid-induced hyperalgesia • May produce a “false positive” result • 50-75% reduction in systemic dose • Liberal use of “breakthrough” medication • Minimal use of “breakthough” medication can be taken as one objective measure of pain relief
IT Bolus (ITB) Vs. Continuous Epidural Infusion (CEI) • 86 patient screened for inclusion • 28 excluded from inclusion • 58 patients approached • 18 declined inclusion • 40 patients randomized • ITB (n=18) or CEI (n=19) • 27 successful trial - pump implantation • ITB, 67% (12/18) CEI, 79% (15/19) • 3 patients lost to follow-up • ITB (n=10), CEI (n=14 Anderson V, Burchiel K, Cooke B: A Prospective Randomized Trial of Intrathecal Injection vs. Epidural Infusion in the Selection of Patients for Continuous Intrathecal Opioid Therapy. Neuromodulation, 2003
IT Bolus Vs. CEI • No significant difference in 6 month outcomes between ITB and CEI • ITB – 60% “successful” response • CEI – 64% “successful” response • Drug-related complications more common in ITB group (88%) vs. CEI group (70%) • CEI 2.5 times more costly ($4,762 vs. 1,862) CONCLUSION: Differences in pain and functional response to long-term IT opioids among patients selected by either trial method are not large
IT Bolus Vs. CEI Anderson V, Burchiel K, Cooke B: A Prospective Randomized Trial of Intrathecal Injection vs. Epidural Infusion in the Selection of Patients for Continuous Intrathecal Opioid Therapy. Neuromodulation, 2003
Complications • Bleeding problems • Spinal epidural hematoma • Pump pocket hematoma/seroma • Infection • most often occurs at pump pocket • REMOVE the system • Post-dural puncture headache • CSF leak • Drug-related side effects • Catheter complications • 20-25% incidence • 20,000 implants annually • 5,000 catheter revisions annually • Estimated revision cost $10,000 • $50,000,000 yearly revision cost
PA03 Update of Clinical Guidelines for the use of Intraspinal Drug Infusion in Pain Management Neuropathic Pain Morphine Hydromorphone Line 1 * Z i c o n o t i d e Morphine (or Hydromorphone) + Bupivacaine Morphine (or Hydromorphone) + Clonidine Line 2 Morphine (or Hydromorphone) + Bupivacaine + Clonidine Line 3 Fentanyl, Sufentanil, Midazolam, Baclofen Line 4 For Selected Patients Only Neostigmine, Adenosine, Ketorolac Line 5 Ropivacaine, Meperidine, Gabapentin, Buprenorphine, Octreotide, other ** Line 6 * The specific line to be determined after FDA review of NDA ** Potential spinal analgesics: Methadone, Oxymorphone, NMDA antagonists
Recommended Maximum Intrathecal Dosages and Concentrations* * These represent general recommendations and are dependent upon the specific patient and the clinical experience of the physician and thus, maximum dosage and/or concentrations may vary from these.
Spinal OpiatesNon-malignant Pain • Mean morphine dose • initial: 2.7 mg/day (0.3-12 mg/day) • after 3.4 years: 4.7 mg/day (0.3-12 mg/day) • 28 patients followed more than 4 years • 64% (n=18) constant dosage history • 36% (n=10) increase in morphine dose > 6mg/day after 1 year Winkellmuller et al.: J Neurosurgery 85:458-467, 1996
Spinal OpiatesNon-Malignant Pain • U.S. experience, 1981-1992 • 14 authors, 156 patients • 69% (107) good-excellent pain relief • 75% with cancer pain – good/excellent pain relief Krames E: Spinal Administration of Opioids for Nonmalignant Pain Syndromes: A U.S. Experience
Spinal Opiates Non-Malignant Pain • 120 patients • 63% (n=76) with FBSS or LBP • Mean age: 54.0 + 11.2 years (28-79) • Follow-up period • mean: 3.4 + 1.3 years (0.5 - 5.7 years) Winkellmuller et al.: J Neurosurgery 85:458-467, 1996
Mean Pain Scores • 74% benefit • Avg. pain reduction • 67% at 6 months • 58% last follow-up • 81% improved QOL • 92% “satisfied” Winkellmuller et al.: J Neurosurgery 85:458-467, 1996
Mean Daily Morphine Dose Winkellmuller et al.: J Neurosurgery 85:458-467, 1996
Multicenter Review of Spinal Opiates • Retrospective review of 429 patients • 66% non-malignant pain • Physician assessment • global pain relief scores • percent pain relief • VAS scores for pain intensity • ADL, overall activity level • Employment Paice: J Pain Symptom Management, 1996
Global Pain Relief • Excellent 52.4% • Good 42.9% • Poor 4.8% Paice: J Pain Symptom Management, 1996
Changes in ADL • Increased 82% • No Change 14% • Decreased 4% Paice: J Pain Symptom Management, 1996
Daily Opiate Dosage • Mean daily dose, 9.2 mg/day • Initial dose higher for non-malignant pain • Gradual linear dose escalation in non-malignant pain • At 24 months, dosages similar in patients with non-malignant and cancer pain Paice: J Pain Symptom Management, 1996
Conclusions of Multicenter Review • Nociceptive pain responds best to spinal opiates • Neuropathic pain responds to spinal opiates but may require higher dosages • Addition of local anesthetics may by synergistic in neuropathic pain
Prospective Study - Spinal Opiates • 40 patients with non-malignant pain • mostly FBSS with > 3 operations • Mean duration of pain, 8 + 9 years (6mos-40yrs) • 30 (75%) had successful screening trial • minimum of 50% pain reduction by VAS • Follow-up 6, 12, 18, 24 months • complete data for 20 patients followed for 2 years • Outcome by VAS, CIPI, BDI, MPQ AndersonV,Burchiel K: Neurosurgery, Feb. 1999
Results • VAS for pain and pain coping scores remained improved • CIPI and MPQ scores improved and persisted • Initial morphine dose 1.96 + 1.8 mg/day, inc. to 6.0 + 7.0 at 3 months, 9.43 + 8.8 at 15 months • Device complications, 20% AndersonV,Burchiel K: Neurosurgery, Feb. 1999
Visual Analog Scores • Mean initial VAS • 78.5 ± 15.9 (39-100) • Decrease in VAS greatest during the initial 3 months • Reduction in VAS remained relatively constant AndersonV,Burchiel K: Neurosurgery, Feb. 1999
Medication Intake • Daily IT morphine dose 25mg • Mean equianalgesic opioid dose increased significantly over time • initial: 1.96 ± 1.75 mg/day • 24 months: 14.59 ± 20.52 mg/day • Dose escalation most rapid during initial 3 months • Oral narcotic intake • initial: 90% (28/30) • 24 months: 30% (6/30) AndersonV,Burchiel K: Neurosurgery, Feb. 1999
Spinal Opiates for Benign PainMaron J, Loeser J: The Clinical Journal Pain, 1996 • Data insufficient to permit formal analysis • The proper role of intraspinal opioids in the treatment of non-malignant pain cannot be determined from the existing literature • Spinal opiates for benign pain should be considered experimental • All patients who receive such therapy should be part of a clinical protocol
Intrathecal Therapy vs. Oral Opioids, vs. Functional Restoration Program for FBSSDoleys, et. al. • Interpretation as to the most effective treatment depends on the outcome measure emphasized. There is a “disconnect” between ratings of pain, disability, mood, and quality of life. The use of a multi-dimensional outcomes approach revealed a number of inconsistencies in the data which could have been overlooked using only pain ratings and patient satisfaction data. No one treatment emerged as the most effective across all of the disease specific and generic measures. Although generally “satisfied” with treatment, patients continued to report significant levels of pain, disability, and impaired quality of life
Unresolved Issues • How should outcome be measured? • Management of tolerance • Question of neurotoxicity • Development of hyperalgesia • Indefinite requirement for medical care
The Bottom Line There can be no substitute for sound clinical judgement based on a detailed assessment of each patient !