Download
1 / 14
160 likes | 224 Views
Anticoagulants are important medications to prevent blood clots and reduce the risk of stroke and heart attack. Learn about injectable and oral anticoagulants, including heparin and enoxaparin, their mechanisms of action, dosages for different conditions, and potential adverse effects.

E N D
Anticoagulants Introduction: Anticoagulants drugs eliminate or reduce the risk of blood clots. They’re often called blood thinners, but these medications don’t really thin your blood. Instead, they help prevent or break up dangerous blood clots that form in your blood vessels or heart. Without treatment, these clots can block your circulation and lead to a heart attack or stroke.
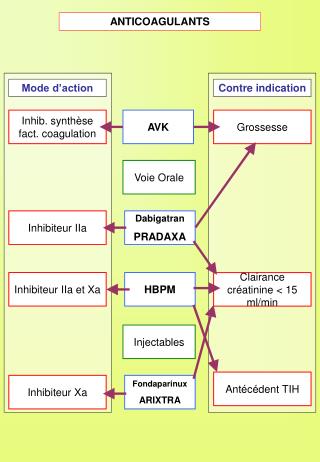
classification • Injectable anticoagulants • Oral anticoagulants
Injectable anticoagulants • 1- Heparin: • Mechanism of Action • Mechanism for low dose: Inactivates factor Xa and inhibits conversion of prothrombin to thrombin • Mechanism for high dose: Inactivates factors IX, X, XI, and XII and thrombin and inhibits conversion of fibrinogen to fibrin • Also inhibits activation of factor VIII • Peak plasma time: 2-4 hr
Metabolism • Metabolized in the liver (partial) and reticuloendothelial system (partial) • Metabolites: None • Elimination • Half-life: 60-90 min average (longer at higher doses) • Dialyzable: No • Excretion: Urine
Dosing: • DVT & PE • Prophylaxis • 5000 units SC q8-12hr, OR • 7500 units SC q12hr • Treatment • 80 units/kg IV bolus, THEN continuous infusion of 18 units/kg/hr, OR • 5000 units IV bolus, THEN continuous infusion of 1300 units/hr, OR • 250 units/kg (alternatively, 17,500 units) SC, THEN 250 units/kg q12hr
Acute Coronary Syndromes • STEMI • Patient on fibrinolytics: IV bolus of 60 units/kg (max: 4000 units), THEN 12 units/kg/hr (max 1000 units/hr) as continuous IV infusion • Dose should be adjusted to maintain aPTT of 50-70 sec • Unstable Angina/NSTEMI • Initial IV bolus of 60-70 units/kg (max: 5000 units), THEN initial IV infusion of 12-15 units/kg/hr (max: 1000 units/hr) • Dose should be adjusted to maintain aPTT of 50-70 sec
Adverse Effects • Heparin-induced thrombocytopenia, possibly delayed (10-30% ) • Frequency Not Defined • Mild pain • Hematoma • Hemorrhage • Local irritation • Erythema • Injection site ulcer (after deep SC injection)
Increased liver aminotransferase • Anaphylaxis • Immune hypersensitivity reaction • Osteoporosis (long-term, high-dose use) • Heparin resistance • Gasping syndrome in infants due to benzyl alcohol preservative • Hypersensitivity
Enoxaparin: • Low molecular weight heparin • Enoxaparin prevents blood clots in patients who are on bed rest or who are having orthopedic surgery of the hip replacement, knee replacement, or large intestinal surgery. It is also used alone or in combination with warfarin to prevent and treat blood clots in the leg.
Clinical use • Deep Vein Thrombosis (Prophylaxis) • Prevent the occurrence of pulmonary embolism in patients at risk for thromboembolic complications who are undergoing abdominal surgery or hip or knee replacement surgery, as well as in medical patients with severely restricted mobility during acute illness
administration • Abdominal surgery • 40 mg SC qDay; initiate 2 hr preoperatively • Knee or hip replacement surgery • 30 mg SC q12hr; initiate therapy 12-24 hr postoperatively and continued for 10 days or up to 35 days postoperatively or until risk of DVT has been significantly reduced or patient is on anticoagulant therapy • For hip replacement surgery, may consider administering 40 mg SC qDay, initiated 9-15 hr preoperatively and continued for 10 days or up to 35 days postoperatively or until risk of DVT has been significantly reduced or patient is on anticoagulant therapy • Medical patients with restricted mobility • 40 mg SC qDay; continue until risk of DVT has been significantly (6-11 days) reduced or patient is on anticoagulant therapy
Deep Vein Thrombosis (Treatment) • Inpatient treatment • Acute DVT with or without PE, when administered in conjunction with warfarin sodium • 1 mg/kg SC q12hr, OR 1.5 mg/kg SC qDay (administer at same time each day) • Continue enoxaparin for a minimum of 5 days and until a therapeutic oral anticoagulant effect has been achieved (INR 2.0-3.0) • Average duration of administration is 7 days; up to 17 days has been administered in clinical trials
Renal impairment • Severe (CrCl <30 mL/min): Dosage reductions required • Prophylaxis in abdominal surgery: 30 mg SC qDay • Prophylaxis in hip or knee replacement surgery: 30 mg SC qDay • Prophylaxis in medical patients with restricted mobility: 30 mg SC qDay • DVT treatment (inpatient or outpatient) coadministered with warfarin: 1 mg/kg SC qDay
Hemorrhage (1-4%) • Elevation of serum aminotransferases (6%) • Fever (5-8%) • Local site reactions (2-5%) • Thrombocytopenia (3%) • Nausea (3%) • Anemia (2%) • Ecchymosis (3%) • <1% • Atrial fibrillation • Heart failure