Download
1 / 37
420 likes | 832 Views
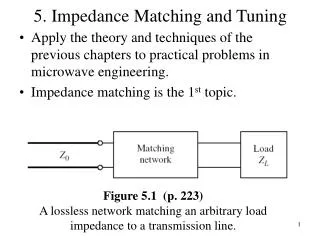
Structurally based HLA matching: A Useful Tool to Fill the Gaps in Current HLA Matching Strategies. Luis G. Hidalgo ATLS Feb. 24, 2010. Review the organization of the MHC and understand the polymorphisms encoded. Outline the differences between current HLA matching and structural HLA matching.

E N D
Structurally based HLA matching: A Useful Tool to Fill the Gaps in Current HLA Matching Strategies Luis G. Hidalgo ATLS Feb. 24, 2010
Review the organization of the MHC and understand the polymorphisms encoded Outline the differences between current HLA matching and structural HLA matching Describe the structural definition of an epitope on an HLA molecule and the algorithms used to define them
The Major Histocompatibility Complex MHC – all mammals Human leukocyte antigen (HLA) - humans
The Major Histocompatibility Complex Class II Class III Class I • DP, DQ, DR • TAP, LMP • C’ proteins • TNF • HLA-A, -B, -C
Polymorphism of HLA Class I and Class II Molecules polymorphism is focused around the peptide binding region Top view of MHC The MHC region is one of the most polymorphic regions of the human genome Polymorphisms help to ensure survival of the species against major pathogen epidemics
Polymorphisms within HLA class I and class II molecules • Effects of the position of MHC polymorphisms: • Possible conformational changes in a helices • Different sets of peptides presented by different MHC molecules
MHC Class I polymorphism The most important HLA class I loci in transplantation are those with the largest number of alleles; HLA-A, -B, and -C
Topography of polymorphic residues on HLA-A/-B/-C molecules HLA-A2 HLA-B27 HLA-Cw3
MHC Class II polymorphism The most important HLA class II loci in transplantation are those with the largest number of alleles; HLA-DR b, -DQ a1 and b1, and –DP a1 and b1
Topography of polymorphic residues on HLA-DR and –DQ molecules HLA-DR HLA-DQ 1 1 1 1 2 2 2 2
MHC polymorphism: the basis for allograft rejection Graft losses increase in proportion to the number of HLA mismatches (MM) despite improved overall survival: 0 MM refers to matching for HLA-A, -B, and –DR only Opelz G. et. al., Transplantation 2007 Is this due to overall increased risk for rejection or increased risk to develop donor specific antibody (DSA)?
De novo DSA is a leading cause for graft loss Graft survival → A major reason for the increased graft loss in proportion to the number of HLA mismatches (MM) is the generation of donor specific antibodies DSA: Graft survival examined according to DSA status of the patient at the time of a clinically indicated biopsy: Hidalgo LG et. al., Am. J. Transpl. 2009
Generation of DSA A1,24; B8 A1,2 B 7,8 + What antibodies are likely to develop?
Generation of DSA A1,24; B8 Anti-A2 A1,2 B 7,8 Anti-B7 +
Generation of DSA A23 A68 A28 B57 Anti A2 A1,24; B8 A69 B58 A1,2 B 7,8 A24 + B42 B55 B47 B13 B48 B27 B60 Anti B7 B61 B54 B41 DSA are rarely generated alone and generally antibodies to HLA molecules related to the donor HLA are also often found: Due to shared epitopes with donor HLA
Current HLA matching for solid organ Recipient and donor are HLA typed at low resolution: 3 Antigen Mismatch (3MM) or 1 class I mismatch + 2 class II mismatches * DP is not currently typed The problem: It is nearly impossible to find 0MM donors using current HLA matching strategy, but many mismatched transplants succeed…
Structural differences between HLA allotypes “Alloimmunized individuals potentially can make an antibody to any HLA epitope that is not present in their own phenotype” HLA Beyond Tears, 2nd Ed, Rodey, 2000
“Seen” by A2,A68; B27,B44 “Seen” by A2,A68; B35,B44 “Seen” by A2,A24; B7,B8 Structural Basis of an HLA-B51 Mismatch Polymorphic Residues on B51 Mismatched HLA antigens have different numbers of mismatched epitopes
Antigen is recognized by the Antibody Combining Site made up ofSix Complementarity-Determining Regions (CDRs): What does an HLA antibody ‘see’ on the HLA molecule?
The antibody combining site Complementarity Determining Regions The antibody combining site includes CDRs from the heavy and light chain: CDR-H1, CDR-H2, CDR-H3, CDR-L1, CDR-L2 and CDR-L3 represent the “binding face” which contacts the structural epitope Antibody specificity is often determined by a centrally located loop (CDR-H3) that binds to the functional epitope a configuration of 3-6 amino acids in the structural epitope; an ‘EPLET’
Structurally based histocompatibility determination • The HLA-A,B,C type of the patient represents six strings of self-eplets that cannot induce specific alloantibodies • Each donor HLA antigen represents a string of eplets • Compatibility is assessed by lining up donor eplet strings with patient eplet strings to determine differences between donor and patient (Microsoft Excel macros program (HLA Matchmaker) – work by Dr. Rene Duquesnoy) Human Immunol. 63: 339-352, 2002 + 63: 353-363, 2002
The HLAMatchmaker algorithm • Considers all surface-exposed polymorphic residues and residues within a 3.0-3.5 Angstrom radius • These polymorphic residues clusters will be referred to as “eplets” and may include nonlinear sequences • Requirement: All well-defined serological determinants should have corresponding eplets
Notation system for eplets The number indicates the amino acid sequence position Polymorphic residues are listed with the single amino acid letter code (monomorphic residues are not listed) Examples: 9F 12SV …. 66RNV 76ES 90A …etc.
The HLA type of the recipient determines what structural components of an immunizing HLA antigen can be “seen” as non-selfHypothesis:Matching at the epitope level provides a better assessment of HLA compatibility than matching at the antigen level Structural Matching Concept
Potential donor has a HLA-B8 mismatch • For which patient is this antigen • a better mismatch? • Patient 1: HLA-A2,A30; B18,B27; Cw2,Cw4 • Patient 2: HLA-A2,A31; B42,B53; Cw2,Cw7
HLA-B8 Mismatch for patient 1(HLA-A2,A30; B18,B27; Cw2,Cw4) Mismatched eplets
HLA-B8 Mismatch for patient 1(HLA-A2,A30; B18,B27; Cw2,Cw4) HLA-B8 has six mismatched eplets with patient 1
HLA-B8 Mismatch for patient 2(HLA-A2,A31; B42,B53; Cw2,Cw7) Patient HLA 9 12 14 17 41 45 56 62 66 70 74 76 80 A2 A*0201 F sV R gR A Me G Ge rKv aHs H Vd gTL A31 A*3101 T sV R gR A Me R Qe rNv aHs iD Vd gTL B42 B*4201 Y sV R gR A Ee G Rn qIy aQa D Es rNl B53 B*5301 Y aM R gR A Te G Rn qIf tNt Y En rIa Cw2 Cw*0202 Y aV R sR A Ge G Re qKy rQa D Vn rKl Cw7 Cw*0701 D aV R gR A Ge G Re qNy rQa aD Vs rNl Donor HLA B8 B*0801 D aM R gR A Ee G Rn qIf tNt D Es rNl
HLA-B8 Mismatch for patient 2(HLA-A2,A31; B42,B53; Cw2,Cw7) 82 90 105 107 127 131 138 142 144 147 149 151 156 158 A2 lRg A W K R T T tKh W aAh aHv L A S A31 lRg A G N R T I tQr W aAr aRv L A S B42 lRg A P G N R M I tQr W aAr aRv D A B53 aLr A P G N S M I tQr W aAr aRv L A Cw2 lRg A P G N R T I tQr W aAr aRe W A Cw7 lRg D P G N R T I tQr L aAr aRa L A B8 lRg A P G N R M I tQr W aAr aRv D A 163 166 171 177 180 184 186 193 199 207 246 248 253 A2 T Ew Y Et Q dA K Av A S A V Q A31 T Ew Y Et Q dP K Av A S S V Q B42 T Ew Y Dt E dP K Pi A G A V E B53 L Ew Y Et Q dP K Pv A G A V E Cw2 E Ew Y Et Q eH K Pv A G A V E Cw7 T Ew Y Et Q eP K Pl A G A V Eq B8 T Ew Y Dt E dP K Pi A G A V E B8 is a zero-eplet mismatch for patient 2
The number of structural mismatches predicts the generation of HLA antibodies Dankers et. al., Transplantation 77: 1236, 2004
Highly sensitized patients: antibodies against the HLA antigens of more than 85% of the panel. Difficult to transplant because cross-match with most donors is positive. Obvious solution: HLA identical or compatible donor but this is of limited success due to inadequate number of donors How to find a suitable donor for these patients? Structural based HLA matching for highly sensitized patients
Structural based matching increases the odds of finding a zero/acceptable mismatch for highly sensitized patients Eurotransplant Patients, Leiden, The Netherlands
Current study Examining the ability of the number of eplet mismatches at HLA-A, -B, -DR, and –DQ to predict the likelihood of developing DSA - ~ 550 patients followed at the U of A Hospital Determine whether thresholds for ISD levels can be set to overcome the potential of developing DSA
Future considerations Structural based HLA matching is optimal with high resolution HLA typing than current standards (including all HLA class II) - allele-specific HLA antibodies, HLA-DP antibodies Some mismatched eplets do not affect reactivity with antibody - can be elucidated based on serum reactivities HLA epitopes have different degrees of immunogenicity - future algorithms must take this variable into account Other CDRs serve as contact sites to stabilize binding to antigen and affect effector function (eg. Complement activation) - next version of HLAMatchmaker calculates eplet mismatches as well as mismatches at 2nd antibody contact site
Acknowledgements Dr. Patricia Campbell Anne Halpin The U of A Hospital Histocompatibility Laboratory staff Dr. Phil Halloran The Alberta Transplant Applied Genomics Centre staff