Download

1 / 47
470 likes | 497 Views
Learn about leucocyte measurement techniques, differential analysis, and cell identification in veterinary diagnostics. Explore how different leucocyte types are identified and their significance in various conditions.

E N D
Leucocytes Kathleen Tennant Clinical Lead, Diagnostic Laboratories
Leucocyte measurement • Most methods use a mixture of impedence properties and optical scatter/ granularity to derive total numbers and a differential • Fluorescence can give another way of differentiating cell types • Information from the graphs can help you to understand how it has derived the differential….
What cell type? • Neutrophils1. • Lymphocytes 2. • Monocytes3. • Eosinophils4. • Basophils 5.
Lymphocyte • Lymphocytes are small compared to the other leucocytes and have round, non- complex nuclei
On this scatter plot • Neutrophils • Lymphocytes • Monocytes • Eosinophils • Basophils are white • Knowing what the cells look like, you can predict their position and see how cleanly the colours are grouped together
Other measures such as granularity and lobularity allow a 5 part differential
What leucocyte type will the green dots be? • Neutrophils1. • Lymphocytes 2. • Monocytes3. • Eosinophils4. • Basophils 5.
What leucocyte type will the green dots be? • Neutrophils • Lymphocytes • Monocytes • Eosinophils! • Basophils are white
Eosinnophils • In dogs and cats the most obviously granular nucleated cells will be eosinophils
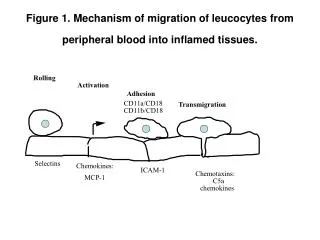
Leucocytes - Neutrophils • Combination of absolute numbers and morphology changes give the best chance of correctly interpreting. • Mature neutrophils in three pools – in circulation, marginated and mature pool in the bone marrow
Mature neutrophilia • By redistribution (marrow to blood stream, marginated to free flowing) in response to inflammatory mediators or increased blood pressure • Decreased loss to tissues in response to corticosteroids often with hypersegmentation
Left shift • Once the mature pool has been stripped from the marrow, if demand outstrips new neutrophil production, earlier precursors released: • Bands, metamyelocytes, myelocytes • (Unusual for promyelocytes/ blasts to be seen in peripheral blood) • Presence indicates an acute inflammatory response that is overwhelming the ability of the marrow to cope
Case 6: 3 y.o. Working Labrador with pyothorax – peripheral blood – what is this cell?
What is this cell? • Lymphocyte, reactive 1 • Monocyte2 • Band neutrophil3 • Metamyelocyte4 • Myelocyte 5
Left shifted neutrophil line • The white arrow shows a myelocyte – reniform, and the earliest in the neutrophil maturation pool
‘Toxic change’ • In response to overwhelming demand, dysmature neutrophils released • Organelles normally removed before the neutrophil is released persist, other organelles not fully matured • Cytoplasmic basophilia, doehle bodies, vacuolation, persistent granules (toxic granulation), ring form nuclei • Often seen alongside left shift
Lasercyte • As immature neutrophils contain more RNA, they occupy a recognisable area of the scatter plot in this technology, but the severity of the left shift and toxic change are best evaluated on the smear
Neutropenia • Breed variations (Greyhounds/ sight hounds) and individual variation: if mild, track. • May be secondary to decreased production with marrow disease/ suppression (esp chemo), increased utilisation with marked inflammation or immune mediated destruction • With complete marrow destruction or suppression, neutrophils are the first cell line to decrease.
Name the cell • Neutrophil1. • Band neutrophil with toxic change 2. • Lymphocyte 3. • Monocyte4.
Monocytes • Have marginated and circulating pools • Leave circulation to tissues, differentiate into macrophages with inflammatory cytokines. • Larger than neutrophils, with a more open nuclear chromatin • Cytoplasm blue – grey and may be vacolated
Monocytosis • Steroids may move them out of the marginated pool • Many infectious causes: bacterial, fungal, protozoal • Immune mediated disease, sepsis, necrosis, trauma • ? systemic studies on prevalence of diagnostic categories with monocytosis as a finding – tend to be case reports/ case series
Lymphocytes • Small, normal lymphocytes in circulation are 1 – 1.5 x red cell size with a thin rim of cytoplasm
Lymphocytes on the blood smear • Reactive lymphocytes • Slightly larger • More basophilic • May have a pale perinuclear zone • Seen more frequently in young animals • May not reflect function
Lymphoblasts • Large lymphoid cells, larger than neutrophils • Their presence in circulation is always abnormal • Look for nucleoli • Generally lymphoma/ leukaemia in high number
Lymphocytosis • Lymphocytosis in physiological response as well as immune stimulation with few diseases (Ehrlichia, Leishmania, Toxoplasma) • Addison’s (5 – 10%) of cases • NOT found as a response to vaccination in various studies (summarised in Avery and Avery (2007) Vet Clin Small Anim37 p267 – 282) • Marked lymphocytosis (> 20 x 10^9/L) raises concerns for neoplasia
Lymphopenia • Lymphopaenia is a common finding • Stressed and diseased animals • Post steroids and some chemotherapeutics
Name that cell • Basophil1. • Toxic neutrophil2. • Eosinophil3. • Macrophage 4.
Eosinophils - eosinophilia • Commonest causes in dogs – pulmonary infiltrate with eosinophils and GI disease (eosinophilic I.B.D.) (Lilliehook and Tvedten, Vet Clin North Am Small AnimPract. 2003 Nov; 33 (6):1359-78 • Eosinophilicleukaemias and paraneoplastic increases also reported • Hypereosinophilic syndrome (huskies) can give marked elevations of well differentiated cells
Eosinophils - eosinopenia • Usually corticosteroid related (endogenous or exogenous) • Insulin administration • Diurnal variation in humans may be reflected in dogs (fewer in the morning)
Name that cell • Basophil1. • Toxic neutrophil2. • Neutrophil containing Ehrlichia3. • Eosinophil4. • Macrophage 5.
Basophils • In hypersensitivity, parasitic and paraneoplastic responses • Basophilic leukaemias reported but rare • Increases in some myelodyplastic syndromes • Dirofilaria in imported • Decreases generally unrecognised
Sample number 3235 • 12 y ME Bulldog • Lethargy, inappetance, mild lymphadenomegaly, splenomegaly • Biochemistry unremarkable
Which is the most likely pathology? • Immune stimulation 1. • Chronic lymphocytic leukaemia 2. • Acute lymphoblastic leukaemia 3. • Stage 5 lymphoma 4.
Lymphocytosis • Cats can have lymphocytosis up to low twenties with immune stimulation • Can not tell whether leukaemia or stage 5 lymphoma based on smear or bone marrow – needs clinical assessment and observation of progression • Morphology on the smear needed to tell if acute (poorly differentiated/ large lymphoid cells) or chronic lymphocytic (small/ well differentiated)
Large granular lymphocytes in very high numbers – suspicious for large granular lymphocyte leukaemia
Large granular lymphoid leukaemia can start in spleen as well as marrow • These lymphocytes can be seen in health and in reactive processes, but not normally in these numbers • High numbers of Howell – Jolly bodies (arrowed) – seen in red cell regeneration (not here!) and in some animals with splenic disease