Download
1 / 1
10 likes | 127 Views
Psychological Distress and Recurrent Pain: Results from the 2002 NHIS Loren Toussaint, Ph.D. & Alyssa Cheadle Luther College, Decorah, Iowa email: touslo01@luther.edu or cheaal01@luther.edu. Method Sample Data from the 2002 National Health Interview Survey (NHIS) were analyzed.

E N D
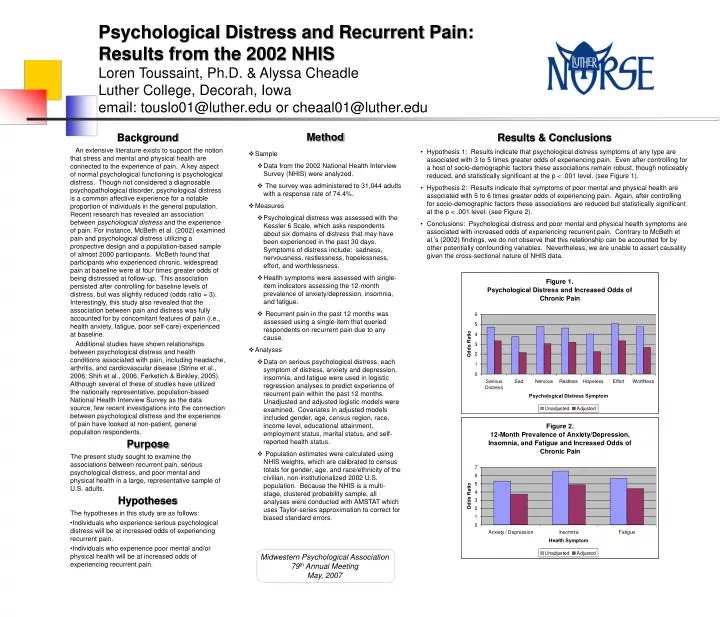
Psychological Distress and Recurrent Pain:Results from the 2002 NHISLoren Toussaint, Ph.D. & Alyssa CheadleLuther College, Decorah, Iowaemail: touslo01@luther.edu or cheaal01@luther.edu • Method • Sample • Data from the 2002 National Health Interview Survey (NHIS) were analyzed. • The survey was administered to 31,044 adults with a response rate of 74.4%. • Measures • Psychological distress was assessed with the Kessler 6 Scale, which asks respondents about six domains of distress that may have been experienced in the past 30 days. Symptoms of distress include: sadness, nervousness, restlessness, hopelessness, effort, and worthlessness. • Health symptoms were assessed with single-item indicators assessing the 12-month prevalence of anxiety/depression, insomnia, and fatigue. • Recurrent pain in the past 12 months was assessed using a single-item that queried respondents on recurrent pain due to any cause. • Analyses • Data on serious psychological distress, each symptom of distress, anxiety and depression, insomnia, and fatigue were used in logistic regression analyses to predict experience of recurrent pain within the past 12 months. Unadjusted and adjusted logistic models were examined. Covariates in adjusted models included gender, age, census region, race, income level, educational attainment, employment status, marital status, and self-reported health status. • Population estimates were calculated using NHIS weights, which are calibrated to census totals for gender, age, and race/ethnicity of the civilian, non-institutionalized 2002 U.S. population. Because the NHIS is a multi-stage, clustered probability sample, all analyses were conducted with AMSTAT which uses Taylor-series approximation to correct for biased standard errors. • Results & Conclusions • Hypothesis 1: Results indicate that psychological distress symptoms of any type are associated with 3 to 5 times greater odds of experiencing pain. Even after controlling for a host of socio-demographic factors these associations remain robust, though noticeably reduced, and statistically significant at the p < .001 level. (see Figure 1). • Hypothesis 2: Results indicate that symptoms of poor mental and physical health are associated with 5 to 6 times greater odds of experiencing pain. Again, after controlling for socio-demographic factors these associations are reduced but statistically significant at the p < .001 level. (see Figure 2). • Conclusions: Psychological distress and poor mental and physical health symptoms are associated with increased odds of experiencing recurrent pain. Contrary to McBeth et al.’s (2002) findings, we do not observe that this relationship can be accounted for by other potentially confounding variables. Nevertheless, we are unable to assert causality given the cross-sectional nature of NHIS data. • Background • An extensive literature exists to support the notion that stress and mental and physical health are connected to the experience of pain. A key aspect of normal psychological functioning is psychological distress. Though not considered a diagnosable psychopathological disorder, psychological distress is a common affective experience for a notable proportion of individuals in the general population. Recent research has revealed an association between psychologicaldistress and the experience of pain. For instance, McBeth et al. (2002) examined pain and psychological distress utilizing a prospective design and a population-based sample of almost 2000 participants. McBeth found that participants who experienced chronic, widespread pain at baseline were at four times greater odds of being distressed at follow-up. This association persisted after controlling for baseline levels of distress, but was slightly reduced (odds ratio = 3). Interestingly, this study also revealed that the association between pain and distress was fully accounted for by concomitant features of pain (i.e., health anxiety, fatigue, poor self-care) experienced at baseline. • Additional studies have shown relationships between psychological distress and health conditions associated with pain, including headache, arthritis, and cardiovascular disease (Strine et al., 2006; Shih et al., 2006; Ferketich & Binkley, 2005). Although several of these of studies have utilized the nationally representative, population-based National Health Interview Survey as the data source, few recent investigations into the connection between psychological distress and the experience of pain have looked at non-patient, general population respondents. • Purpose • The present study sought to examine the associations between recurrent pain, serious psychological distress, and poor mental and physical health in a large, representative sample of U.S. adults. • Hypotheses • The hypotheses in this study are as follows: • Individuals who experience serious psychological distress will be at increased odds of experiencing recurrent pain. • Individuals who experience poor mental and/or physical health will be at increased odds of experiencing recurrent pain. Midwestern Psychological Association 79th Annual Meeting May, 2007






















