Download
1 / 1
10 likes | 88 Views
Reducing the Effects of Ventricular Septal Defects, Hypertrophic Cardiomyopathy, and Coronary Heart Disease Amalia Kondyles, Madison Pace, Michael Wyngarden College of Agriculture and Life Sciences, North Carolina State University. Abstract

E N D
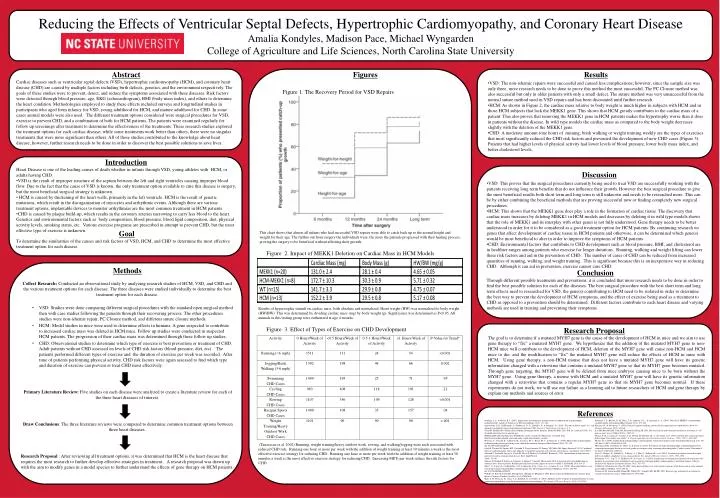
Reducing the Effects of Ventricular Septal Defects, Hypertrophic Cardiomyopathy, and Coronary Heart DiseaseAmalia Kondyles, Madison Pace, Michael Wyngarden College of Agriculture and Life Sciences, North Carolina State University Abstract Cardiac diseases such as ventricular septal defects (VSD), hypertrophic cardiomyopathy (HCM), and coronary heart disease (CHD) are caused by multiple factors including birth defects, genetics, and the environment respectively. The goals of these studies were to prevent, detect, and reduce the symptoms associated with these diseases. Risk factors were detected through blood pressure, age, EKG (echocardiogram), BMI (body mass index), and others to determine the heart condition. Methodologies employed to study these effects included surveys and longitudinal studies in participants who aged from infancy for VSD, young adulthood for HCM, and mature adulthood for CHD. In some cases animal models were also used. The different treatment options considered were surgical procedures for VSD, exercise to prevent CHD, and a combination of both for HCM patients. The patients were examined regularly for follow up screenings after treatment to determine the effectiveness of the treatments. These research studies explored the treatment options for each cardiac disease; while some treatments work better than others, there were no singular treatments that were more significant than others. All of these studies contributed to the knowledge about heart disease; however, further research needs to be done in order to discover the best possible solutions to save lives. Figures • Results • VSD: The non-ishemic repairs were successful and caused less complications; however, since the sample size was only three, more research needs to be done to prove this method the most successful. The PC Closure method was also successful but only in older patients with only a small defect. The suture method was very unsuccessful from the normal suture method used in VSD repairs and has been discounted until further research. • HCM: As shown in Figure 2, the cardiac mass relative to body weight is much higher in subjects with HCM and in those HCM subjects that lack the MEKK1 gene. This shows that HCM greatly contributes to the cardiac mass of a patient. This also proves that removing the MEKK1 gene in HCM patients makes the hypertrophy worse than it does in patients without the disease. In wild type models the cardiac mass as compared to the body weight decreases slightly with the deletion of the MEKK1 gene. • CHD: A moderate amount (one hour) of running, brisk walking or weight training weekly are the types of exercises that most significantly reduced the CHD risk factors and prevented the development of new CHD cases (Figure 3). Patients that had higher levels of physical activity had lower levels of blood pressure, lower body mass index, and better cholesterol levels. Figure 1. The Recovery Period for VSD Repairs • Introduction • Heart Disease is one of the leading causes of death whether in infants through VSD, young athletes with HCM, or adults having CHD. • VSD is the result of improper structure of the septum between the left and right ventricles causing improper blood flow. Due to the fact that the cause of VSD is known, the only treatment option available to cure this disease is surgery, but the most beneficial surgical strategy is unknown. • HCM is caused by thickening of the heart walls, primarily in the left ventricle. HCM is the result of genetic mutations, which result in the disorganization of myocytes and arrhythmic events. Although there are various treatment options, implantable devices to monitor arrhythmias are the most common treatment in HCM patients. • CHD is caused by plaque build-up, which results in the coronary arteries narrowing to carry less blood to the heart. Genetics and environmental factors such as body composition, blood pressure, blood lipid composition, diet, physical activity levels, smoking status, etc. Various exercise programs are prescribed in attempt to prevent CHD, but the most effective type of exercise is unknown. Discussion • VSD: This proves that the surgical procedures currently being used to treat VSD are successfully working with the patients receiving long term benefits that do not influence their growth. However the best surgical procedure to give the most beneficial results both short term and long term is still unknown and needs to be researched more. This can be by either combining the beneficial methods that are proving successful now or finding completely new surgical procedures. • HCM: This shows that the MEKK1 gene does play a role in the formation of cardiac tissue. The discovery that cardiac mass increases by deleting MEKK1 in HCM models and decreases by deleting it in wild type models shows that the role of MEKK1 and its interplay with other genes is not fully understood. Gene therapy needs to be better understood in order for it to be considered as a good treatment option for HCM patients. By continuing research on genes that affect development of cardiac tissue in HCM patients and otherwise, it can be determined which gene(s) would be most beneficial to alter in order to improve the symptoms of HCM patients. • CHD: Environmental factors that contribute to CHD development such as blood pressure, BMI, and cholesterol are in healthier ranges among patients who exercise for longer durations. Running, walking and weight lifting can lower these risk factors and aid in the prevention of CHD. The number of cases of CHD can be reduced from increased quantities of running, walking, and weight training. This is significant because this is an inexpensive way in reducing CHD. Although it can aid in prevention, exercise cannot cure CHD. Goal To determine the similarities of the causes and risk factors of VSD, HCM, and CHD to determine the most effective treatment option for each disease. This chart shows that almost all infants who had successful VSD repairs were able to catch back up to the normal height and weight for their age. The further out from surgery the individuals were, the more the patients progressed with their healing process, proving the surgery to be beneficial without affecting their growth. Figure 2. Impact of MEKK1 Deletion on Cardiac Mass in HCM Models • Methods • Collect Research: Conducted an observational study by analyzing research studies of HCM, VSD, and CHD and the various treatment options for each disease. The three diseases were studied individually to determine the best treatment option for each disease. • VSD: Studies were done comparing different surgical procedures with the standard open surgical method then with case studies following the patients through their recovering process. The other procedures studies were non-ishemic repair, PC Closure method, and different suture closure methods. • HCM: Model studies in mice were used to determine effects in humans. A gene suspected to contribute to increased cardiac mass was deleted in HCM mice. Follow up studies were conducted in suspected HCM patients. The progression of their cardiac mass was determined through these follow up studies. • CHD: Observational studies to determine which type of exercise is best prevention or treatment of CHD. Adult patients without CHD assessed on levels of CHD risk factors (blood pressure, diet, etc) . The patients performed different types of exercise and the duration of exercise per week was recorded. After time of patients performing physical activity, CHD risk factors were again assessed to find which type and duration of exercise can prevent or treat CHD most effectively. • Primary Literature Review: Five studies on each disease were analyzed to create a literature review for each of the three heart diseases of interest. • Draw Conclusions: The three literature reviews were compared to determine common treatment options between three heart diseases. • Research Proposal : After reviewing all treatment options, it was determined that HCM is the heart disease that requires the most research to further develop effective strategies in treatment.. A research proposal was drawn up with the aim to modify genes in a model species to further understand the effects of gene therapy on HCM patients. Conclusion Through different possible treatments and preventions, it is concluded that more research needs to be done in order to find the best possible solution for each of the diseases. The best surgical procedure with the best short term and long term effects need to researched for VSD, the gene(s) contributing to HCM need to be isolated in order to determine the best way to prevent the development of HCM symptoms, and the effect of exercise being used as a treatment to CHD as opposed to a prevention should be determined. Different factors contribute to each heart disease and varying methods are used in treating and preventing their symptoms. Results of hypertrophic stimuli on cardiac mass, both absolute and normalized. Heart weight (HW) was normalized to body weight (HW/BW). This was determined by dividing cardiac mass (mg) by body weight (g). Significance was determined as P<0.05. All animals in this testing group were euthanized at age 4 months. Figure 3. Effect of Types of Exercise on CHD Development Research Proposal The goal is to determine if a mutated MYH7 gene is the cause of the development of HCM in mice and we aim to use gene therapy to “fix” a mutated MYH7 gene. We hypothesize that the addition of the mutated MYH7 gene to non-HCM mice will contribute to the development of HCM, deletion of the MYH7 gene will cause non-HCM and HCM mice to die, and the modification to “fix” the mutated MYH7 gene will reduce the effects of HCM in mice with HCM. Using gene therapy, a non-HCM mouse that does not have a mutated MYH7 gene will have its genetic information changed with a retrovirus that contains a mutated MYH7 gene so that its MYH7 gene becomes mutated. Through gene targeting, the MYH7 gene will be deleted from mice embryos causing mice to be born without the MYH7 gene. Using gene therapy, a mouse with HCM and a mutated MYH7 gene will have its genetic information changed with a retrovirus that contains a regular MYH7 gene so that its MYH7 gene becomes normal. If these experiments do not work, we will use our failure as a learning aid to future researchers of HCM and gene therapy by explain our methods and sources of error. References • Adabag, A. S., & Maron, B. J. (2007). Implications of arrhythmias and prevention of sudden death in hypertrophic cardiomyopathy. Annals of Noninvasive Electrocardiology, 12(2), 171-180. • Apostolakis, E. E., Kallikourdis, A., Baikoussis, N. G., Dedeilias, P., & Dougenis, D. (2010). "The non-ischemic repair" as a safe alternative method for repair of anterior post-infarction VSD. Journal of Cardiothoracic Surgery, 5, 6. • Chen M. Medline Plus Medical Encyclopedia [homepage on the Internet]. Bethesda (MD): 2011 Feb. 28. [cited 2011 Feb. 10]. Available from http://www.nlm.nih.gov. • EMedicineHealth.com [Internet]. WebMd, Inc; c2011. [citied 2011 March 12]. Available from: http://www.emedicinehealth.com/ventricular_septal_defect/article_em.htm • Frustaci, A., Verardo, R., Caldarulo, M., Acconcia, M. C., Russo, M. A., & Chimenti, C. (2007). Myocarditis in hypertrophic cardiomyopathy patients presenting acute clinical deterioration. European Heart Journal, 28(6), 733-740. doi:10.1093/eurheartj/ehl525 • Goel K, Thomas RJ, Squires RW, Coutinho T, Trejo-Gutierrez JF, Somers VK, Miles JM, Lopez-Jimenez F. 2011. Combined effect of cardiorespiratory fitness and adiposity on mortality in patients with coronary artery disease. Am Heart J 161(3):590-7. • Guiraud T, Juneau M, Nigam A, Gayda M, Meyer P, Mekary S, Paillard F, Bosquet L. 2010. Optimization of high intensity interval exercise in coronary heart disease. Eur J ApplPhysiol • 108(4):733-40. • Hansen D, Dendale P, Raskin A, Schoonis A, Berger J, Vlassak I, Meeusen R. 2010. Long-term effect of rehabilitation in coronary artery disease patients: Randomized clinical trial of the impact of exercise volume. ClinRehabil 24(4):319-27. • Ho, C. Y., Lopez, B., Coelho-Filho, O. R., Lakdawala, N. K., Cirino, A. L., Jarolim, P., et al. (2010). Myocardial fibrosis as an early manifestation of hypertrophic cardiomyopathy. The New England Journal of Medicine, 363(6), 552-563. doi:10.1056/NEJMoa1002659 • Jolliffe JA, Rees K, Taylor RS, Thompson D, Oldridge N, Ebrahim S. 2000. Exercise-based rehabilitation for coronary heart disease. Cochrane Database Syst Rev (4)(4):CD001800. • Kale, S. B., Finucane, K., Chan, T. L., Rumball, E., & Gentles, T. (2010). Midterm results of repair of perimembranous or conal ventricular septal defects using the transaortic direct suture technique. The Annals of Thoracic Surgery, 89(4), 1244 1249. • Konhilas, J. P., Boucek, D. M., Horn, T. R., Johnson, G. L., & Leinwand, L. A. (2010). The role of MEKK1 in hypertrophic cardiomyopathy. International Heart Journal, 51(4), 277-284. • Kuciene, R., & Dulskiene, V. (2010). Parental cigarette smoking and the risk of congenital heart septal defects.Medicina (Kaunas, Lithuania), 46(9), 635-641. • Lee IM, Rexrode KM, Cook NR, Manson JE, Buring JE. 2001. Physical activity and coronary heart disease in women: Is "no pain, no gain" passe? JAMA 285(11):1447-54. • Manso, P. H., Carmona, F., Jacomo, A. D., Bettiol, H., Barbieri, M. A., & Carlotti, A. P. (2010). Growth after ventricular septal defect repair: Does defect size matter? A 10-year experience.ActaPaediatrica (Oslo, Norway : 1992), 99(9), 1356-1360. • Maron, B. J. (2009). Sudden death in hypertrophic cardiomyopathy. Journal of Cardiovascular Translational Research, 2(4), 368-380. doi:10.1007/s12265-009-9147-0 • Movahed, M. R., Strootman, D., Bates, S., & Sattur, S. (2010). Prevalence of suspected hypertrophic cardiomyopathy or left ventricular hypertrophy based on race and gender in teenagers using screening echocardiography. Cardiovascular Ultrasound, 8, 54. doi:10.1186/1476-7120-8-54 • Oses, P., Hugues, N., Dahdah, N., Vobecky, S. J., Miro, J., Pellerin, M., et al. (2010). Treatment of isolated ventricular septal defects in children: Amplatzer versus surgical closure. The Annals of Thoracic Surgery, 90(5), 1593-1598. • Puntmann, V. O., Yap, Y. G., McKenna, W., & Camm, A. J. (2010). Significance of maximal and regional left ventricular wall thickness in association with arrhythmic events in patients with hypertrophic cardiomyopathy. Circulation Journal : Official Journal of the Japanese Circulation Society, 74(3), 531-537. • Talbot LA, Weinstein AA, Fleg JL. 2009. Army physical fitness test scores predict coronary heart disease risk in army national guard soldiers. Mil Med 174(3):245-52. • Tanasescu M, Leitzmann MF, Rimm EB, Willett WC, Stampfer MJ, Hu FB. 2002. Exercise type and intensity in relation to coronary heart disease in men. JAMA 288(16):1994-2000. (Tanasescu et al. 2002) Running, weight training/heavy outdoor work, rowing, and walking/jogging were each associated with reduced CHD risk. Running one hour or more per week with the addition of weight training at least 30 minutes a week is the most effective exercise strategy for reducing CHD. Running one hour or more per week with the addition of weight training at least 30 minutes a week is the most effective exercise strategy for reducing CHD. Increasing METs per week reduce the risk factors for CHD.



















