Download
1 / 19
190 likes | 285 Views
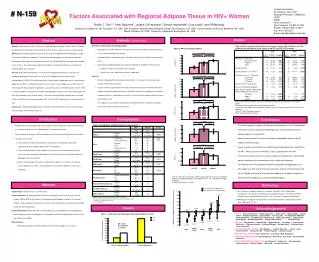
Factors Associated with HIV Education Attendance. R. Sterling, S. Weinstein, P. Crits-Cristoph, D.A. Calsyn, S. R. Doyle. Abstract.

E N D
Factors Associated with HIV Education Attendance R. Sterling, S. Weinstein, P. Crits-Cristoph, D.A. Calsyn, S. R. Doyle
Abstract Substance abusers are known to be at increased risk for HIV transmission. Recognizing this, NIDA, through its Clinical Trials Network recently undertook a study of the relative efficacy of a five-session gender specific intervention, Real Men Are Safe (REMAS), versus a single HIV/AIDS education (i.e., control) session, for current male patients enrolled in either methadone maintenance treatment (MMTP) or outpatient drug-free (ODF) care. The accumulating literature that indicates that HIV transmittal risk can be reduced through increased education led us to examine whether study entry factors that contribute to premature intervention termination could be identified. Subjects were 570 males evenly distributed across MMTP and ODF conditions; 282 were randomly assigned to the five-session REMAS intervention. Overall attendance at the group sessions was disappointing. Attendance to the one session control group was 57%. Only 52% of patients assigned to the REMAS condition attended 3 or more groups. A series of logistic regressions undertaken to examine the influence of study entry measures, including demographic factors such as age, race, years of education, marital status as well as attitude toward condom use indicated that the only significant predictor of intervention attendance/completion was enrollment in methadone maintenance treatment for attendance at the REMAS sessions.
Background • Prendergrast et al. (2001) conducted a meta-analysis of substance abuse treatment-based HIV risk reduction interventions and found significant support for their efficacy. Of particular interest were the findings that intensity of the intervention (i.e., number of sessions) and the use of separate sessions for male and female subjects moderated the overall positive effects. Gibson et al. (1998) had previously observed similar effects of enhanced education. • These findings, as well as those from the NIMH funded Project Light HIV prevention intervention, which in a controlled fashion compared single and multi-session HIV education interventions, contributed to the overall decision to use NIDA’s Clinical Trials Network to evaluate the effectiveness of a gender specific single session HIV education intervention with a more intense, 5 session intervention. • Unfortunately, many individuals terminate treatment prematurely often failing to obtain both the salutary effects of treatment directed at substance reduction as well as the full benefit of HIV education (Metzger, Navaline, & Woody, 1998). • Given the myriad of negative outcomes that have frequently befall the premature substance abuse treatment terminator (Alford, Koehler, & Leonard, 1991; Gottheil, McLellan, & Druley, 1992; Gottheil, Sterling, & Weinstein, 1997; Kelly & Moos, 2003; Kosten, Rounsaville, & Kleber, 1986; Villano, Rosenblum, Magura, & Fong, 2002), the primary goal of this study was to determine if behavioral/psychosocial data of interest collected during entry into a CTN sponsored study of gender-specific HIV education could satisfactorily predict premature intervention termination.
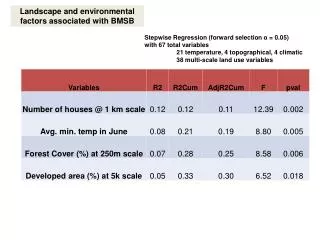
Methods Subjects. Men enrolled in one of 14 substance abuse treatment programs across the US (see Figure 1) were recruited to take part in an HIV/STI prevention project specifically tailored for men (NIDA Clinical Trials Network Protocol 0018). Inclusion criteria included age of 18 or more, engagement in unprotected vaginal or anal intercourse in the prior 6 months, willingness to attend HIV/STI prevention groups and complete assessments at baseline and at 2 wk., 3 mo., 6 mo. post intervention. Exclusion criteria included having a primary partner planning to get pregnant or a Mini Mental Status Exam < 25. Two-thirds of men screened for inclusion met eligibility criteria (see Figure 2). Primary reasons for exclusion were either an absence of sexually activity or condom use 100% of the time for vaginal or anal sex. Primary reason eligible participants were not randomized was loss of contact, usually reflecting leaving treatment. This report focuses on the 570 (96%) of 594 participants randomized to an intervention condition and for whom complete data for conducting the analyses described below are available. Demographics for the sample are provided in Table 1.
Figure 1: Treatment Sites Red=PsychosocialOutpatient Black=Methadone Maintenance Seattle Norwalk Hartford Staten Is. Philadelphia (x2) Toledo Huntington San Francisco Greensboro Raleigh Richmond Santa Fe Rancho Cucamonga
Figure 2: Screening, Baseline & Randomization No Contact other Other 100% condom use Withdrew Pregnancy Planned Left Tx No sex Randomized Eligible MMSE < 25
Methods, cont. Procedures. The study schema is presented in Figure 3. This report focuses on attendance at the assigned HIV prevention intervention sessions. Data of interest collected from the baseline assessment were used to identify variables thought to be associated with attendance at the therapy sessions. Variables of interest came from the demographic questionnaire, ASI, CIDI, Condom Barriers Scale, and the Sexual Behavior Inventory (SBI) and were collected during an extensive structured interview concerning sexual behavior that was administered to eligible subjects via audio computer assisted interview (ACASI) methodology. The two therapy conditions are described briefly in Tables 2 & 3. The HIV Education condition (control) is a 60 minute didactic presentation developed to represent what most programs report already providing in the way of HIV prevention. Real Men Are Safe (REMAS, experimental) is composed of five 90 minute sessions covering the topics listed in Table 3. In Table 4 are listed the different techniques used within the two conditions.
Figure 3: Study Schema Advertise Study Availability Consent to Screen for Inclusion/Exclusion &Screening Assessment Obtain Informed Consent from Eligible Participants Conduct Baseline Assessment→ Place in Waiting Cohort Randomly Assign Cohort to Intervention Standard HIV Education Gender Specific Intervention (one session) (five sessions) Conduct Post Intervention Assessment Conduct Three Month Follow Up Assessment Conduct Six Month Follow Up Assessment
Table 2: HIV Education Outline (Control Group) I. Group Introductions. Goals and Guidelines 5 Min II. HIV/AIDS Update 10 Min III. HIV Risky Behaviors, injection practices 5 Min IV. HIV Risky Behaviors, sexual practices 10 Min V. Healthy Options 10 Min VI. Condom demonstration 10 Min VII. Overcoming Barriers to Condom Use 10 Min
Table 3: Real Men are Safe (REMAS) Outline 1. HIV/AIDS Update: Identifying Risks 2. HIV/AIDS Update: Planning Prevention 3. Sex without drugs. Can it happen? Is it pleasurable? 4. Beyond the pick up line, communicating about sex 5. Communicating about Safe Sex II. Workshop Summary
Table 4: Techniques Utilized in the HIV Education & REMAS HIV Education Lecture Information on Flipcharts Condom Demonstrations REMAS Lecture & Discussion Information on Flipcharts Condom Demonstrations & Practice Brainstorming & Discussion Self Assessment Exercises Role Plays
Methods, cont. Data Analysis. The session attendance rates are provided in Figure 4. For the logistic regression analyses participants were coded as completing REMAS if they attended three or more sessions. Defining REMAS completion as attending 3 or more sessions was based on the investigators a priori clinical experience that exposure to 3 or more REMAS sessions would be sufficiently different from exposure to the control condition to warrant including them in a post hoc “completer analysis” of the primary outcome variable. This definition is similar to that used in Project Light” in which attendance at 5 or more of 7 experimental sessions was defined as completing. Four logistic regressions were conducted, two for each therapy condition, to identify variables associated with attendance at the intervention sessions. The independent variables in one set of analyses included demographic, drug of choice (stimulant/non-stimulant), days of psychological problems in past 30 (ASI), and treatment program type. The independent variables in the other set of analyses included partner sexual risk (high/low), times engaging in sex under the influence in the past 90 days, times engaging in unprotected sex in the past 90 days, attitude towards condoms and treatment program type.
Figure 4: Treatment Exposure HIV-ED REMAS 56.57% 51.56%
Results 1. Overall attendance at the group sessions was disappointing. The proportion of individuals attending the one session HIV-Education (i.e., control) group was 57.6%. In the REMAS condition, the proportion of participants who attended 3 or more session was 51.6% (See Figure 4). 2. Presented in Table 5 is the summary table for the logistic regression predicting REMAS attendance using primarily demographic variables. The model was statistically significant. Being in methadone maintenance had the highest association with REMAS attendance. Reporting more days of psychological distress and not being a stimulant user were also associated with REMAS attendance. 3. However, the second model for REMAS attendance using primarily sexual risk variables was not significant. 4. Neither logistic regression model for HIV Education group attendance was significant. 5. Presented in Figure 5 are the attendance rates as a function of program type. Consistent with the logistic regression analyses, methadone participants have better attendance at the REMAS sessions.
Table 5: Significant Predictors of Attendance at REMAS Group (N=282)
Conclusions • Several interesting findings have emerged from this preliminary study of factors associated with HIV education session attendance: • “Completion” rates observed across the two study conditions (REMAS versus one session control) were disappointing. In this research study patients were not offered “make-up” sessions if they failed to attend the scheduled group. Attendance rates may have been higher if make-ups had been offered. • Interestingly, none of the study entry psychosocial/attitudinal measures, or type of care (i.e., methadone/drug-free) significantly predicted non-attendance in the one session HIV education condition. • With respect to participants assigned to the enhanced, five-session REMAS condition, being enrolled in methadone maintenance as opposed to drug-free outpatient treatment was a significant predictor of “completion” (i.e., 3 or more sessions).
Conclusions, cont. • Fewer ASI recorded number of days of psychological distress in the month prior to study entry was associated with a greater likelihood of attending 3 or more REMAS sessions. • Consistent with the findings of Booth et al (2003), testing positive for a stimulant at study entry (i.e., cocaine, amphetamine) was predictive of failure to complete the REMAS intervention. • Premature treatment termination remains a vexing problem for the substance abuse treatment community. The ability to identify individuals who at treatment initiation are at increased risk for dropout remains a reasonable goal.