Download
1 / 22
290 likes | 644 Views
Bariatric Surgery. Mr Peter O’Leary. History. Greek Baros = weight Iatros = physician Kremen & Linner 1954 Jejuno-ileal Bypass Mason 1967 Gastric Bypass Failure to gain weight post partial gastrectomy for peptic ulcer disease. Recognised as a general surgical sub-speciality by

E N D
Bariatric Surgery Mr Peter O’Leary
History • Greek • Baros = weight • Iatros = physician • Kremen & Linner • 1954 Jejuno-ileal Bypass • Mason • 1967 Gastric Bypass • Failure to gain weight post partial gastrectomy for peptic ulcer disease
Recognised as a general surgical sub-speciality by American College of Surgeons American Medical Association
Mrs. KG (48) • Referred by Orthopaedics re Gastric bypass for: • Weight reduction prior to hip replacement (OA) • Improvement of mobility • Seeking procedure for 4 year • Current status Weight 135kg Height 1.75m BMI 47
HxPC • >9st until mid 20s • Gained weight since the birth of her children • Weight reduction measures • Weight watchers • Dieticians • Appetite suppressants • All effective short term
MedHx • Osteoarthritis B/L hip • Hypertension • Hypercholestrolaemia • Sleep apnoea • Reflux and heart burn • NIDDM
Family Hx Nil of note Drug Hx NKDA Metformin Atenolol SHx Non-smoker No alcholo Shop assistant RoS Nil of note
On Examination • Looked well but obese • Vitals normal • MSS Fixed flexion R knee Joint line tender medially Crepitus + • CVS, RS, Neuro - NAD
Pre-op Advice • Advised about Procedure Possible complication Post-op recovery • Endocrine assessment • No pre-op consultation with Dietician • No pre-op psychological evaluation
Indications • BMI > 40 (> 35 with co-morbid conditions) • sleep apnea • cardiomyopathy • diabetes mellitus • musculoskeletal • body size severely impacting on function • No medical or anaesthetic contraindications • No previous major upper abdominal surgery • No active drug or alcohol addiction history • No major psychiatric history • Well informed, motivated, and acceptable operative risks
Pre-op Considerations • Endocrinologist • Pituitary • Thyroid • Adrenal • Dietician • Eating behaviour modification • Post op diet adjustment, vitamin and mineral supplementation • Psychological evaluation • Psychiatric co-morbidities • Change in relationship with food • Behaviour modification techniques
Bariatric surgery • weight reduction surgery for morbidly obese 1.BMI >40 (basically, >100 pounds above ideal body weight). 2.BMI >35 with a medical problem related to morbid obesity.
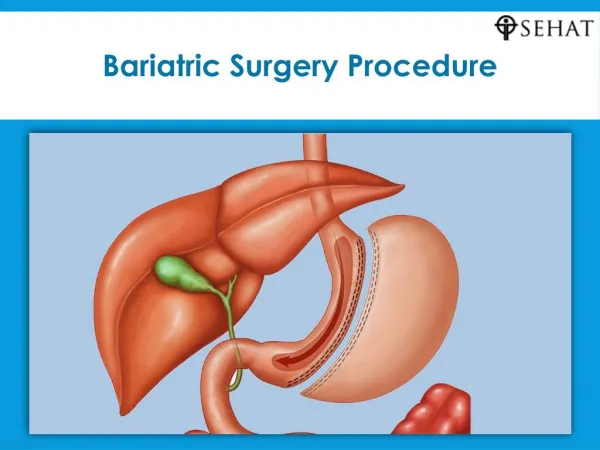
Surgical options • Stapling off of small gastric pouch (restrictive) roux-en-Y limb to gastric pouch
Mechanism of gastric by pass • 1. Creates a small gastric reservoir • 2. Causes dumping symptoms when a patient eats too much food or high calorie foods, the food is dumped into the roux-en-Y limb • 3. Bypass of small bowel by roux-en-Y limb
Dose gastric by pass work? • Weight loss 50% of excess weight
Postop Complications Leak after gastric bypass on upper gastrointestinal series • Early (1 to 6 weeks) • Postoperative bleeding • Anastomosis leak • Bowel perforation • Bowel obstruction • Wound infections • Intermediate (7 to 12 weeks) • Prolonged vomiting • Dietary indiscretions • Bulimia • Stricture at gastrojejunal anastomosis (4.6%) • Marginal ulcer • Dumping syndrome (50% after roux en y) • Late (13 weeks to 12 months) • Cholelithiasis • Small bowel obstruction (adhesions) • Secondary hyperparathyroidism
Long term eating habits • Initially, the stomach tolerates 30 cc at one time • 3 months, patients are ingesting ~1000 kcal in three to six meals per day • Dietary advice important at this stage • Six months, should be on 3 meals a day • Food aversions develop esp if prolonged vomiting associated with eating • Such patients often express "buyers remorse" and may request extensive investigations for problems with the gastric pouch • Eating habits change compared to preoperative eating habits • Fresh fruits and vegetables are tolerated without a problem • Some patients have continuing food intolerances, especially to red meat, and become vegetarian
Changes post surgery • Weight loss • Rapid in the first six months • Averages 4 to 7 Kg per month • Slows 2 to 3 Kg after 6 months • Total weight loss peaks at 12 months • Weight regain 18-24 months post op • Nutritional Deficiencies • Inadequate intake of nutrients • Alterations in the digestive anatomy • lack of intrinsic factor – B12 def • Lack of acid in new pouch (R en Y) – Poor absorption of iron • Ca and Vit D absorption decreased after surgery – Secondary Hyperthyroidism • Thiamine def due to recurrent vomiting • Little evidence available on the amount of supplementation required
Cosmetic • After 12 months, patients seek info about plastic surgery to remove abdominal pannus • Insurance companies will not cover it - cosmetic • Exception if abdominal pannus becomes infected or excoriated • Case series suggested that delaying panniculectomy until after weight loss is safer and more effective • Physical function • Fatigue improves, increased energy • Exercise habits improve • increase in activities of daily living and recreational activities • Musculoskeletal and back pain improves or resolves in the majority of patients • Osteoarthritis improves to a lesser degree • Dependent on the degree of underlying bone and cartilage damage • Sleep apnea improves
Psychological • Lethargy, depression, and other psychopathology • Food used for emotional reasons, pre-op • Grieve the loss of food • Several studies have shown increases in self-esteem, self-confidence, assertiveness, and expressiveness • Improvements seen in social interaction, sexual activity, and work performance • Pregnancy • Greater fertility with weight loss • Surgery not associated with adverse perinatal outcomes • Pregnancy complications eg gestational diabetes, hypertension, and macrosomia • Period of rapid weight loss • Gastric band may need to be adjusted • nutritional deficiencies
"un poco con la cabeza de Maradona y otro poco con la mano de Dios"