Download
1 / 33
370 likes | 698 Views
Bariatric Surgery. Kevin M. Reavis, MD FACS Esophageal, Foregut & Bariatric Surgery The Oregon Clinic. LEGACY WEIGHT & DIABETES INSTITUTE. Relevant Disclosures. None. Objectives. Objectives: To determine appropriate candidates for primary bariatric surgery

E N D
Bariatric Surgery Kevin M. Reavis, MD FACS Esophageal, Foregut & Bariatric Surgery The Oregon Clinic LEGACY WEIGHT & DIABETES INSTITUTE
Relevant Disclosures None
Objectives • Objectives: • To determine appropriate candidates for primary bariatric surgery • To understand the three major types of bariatric surgical procedures offered • To understand the surgical and endoscopic indications for revision bariatric surgery
Specifics today • Epidemiology of obesity • Evaluation of the obese patient • Medical & surgical treatments • Outcomes • Emerging treatments
Classification of Obesity • Overweight 25-29.9 kg/m2 • Obese 30-34.9 kg/m2 • Severe Obesity 35-39.9 kg/m2 • Morbid Obesity 40-49.9 kg/m2 • Super Obesity 50-59.9 kg/m2 • Super-Super Obesity 60+ kg/m2
“Patients who are naturally very fat are apt to die earlier than those who are slender” Hippocrates, 460-377 BC
Obesity Trends* Among U.S. AdultsBRFSS, 1985 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14%
Obesity Trends* Among U.S. AdultsBRFSS, 1995 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14% 15%–19%
Obesity Trends* Among U.S. AdultsBRFSS, 2000 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14% 15%–19% ≥20%
Obesity Trends* Among U.S. AdultsBRFSS, 2005 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) <10% 10%–14% 15%–19% 20%–24% 25%–29% ≥30%
Obesity Trends* Among U.S. AdultsBRFSS, 2009 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14% 15%–19% 20%–24% 25%–29% ≥30%
Current U.S. Statistics • 58 Million overweight • 40 Million obese • 3 Million morbidly obese • 400,000 related deaths annually • > $25 Billion in annual healthcare costs
Cultural Diversity:High Risk Populations • Pima Indians • Polynesians • African American • Latino American • Lower socioeconomics: • Difficulty accessing care • $$$ for healthy foods
Age • 30-50% of Adults • Adolescents: 15-25% • Bimodal distribution… today’s adolescents are tomorrow’s adults
Comorbidities Pulmonary disease abnormal function asthma obstructive sleep apnea hypoventilation syndrome Idiopathic intracranial hypertension Stroke Cataracts Nonalcoholic fatty liver disease steatosis steatohepatitis cirrhosis Coronary heart disease Diabetes Dyslipidemia Hypertension Gall bladder disease Gynecologic abnormalities abnormal menses infertility polycystic ovarian syndrome Severe pancreatitis Cancer breast, uterus, cervix colon, esophagus, pancreas kidney, prostate Osteoarthritis Skin Phlebitis venous stasis Gout
Diabetic Metabolic Syndrome • Non-insulin dependent diabetes (type II) • Hypertension • Dyslipidemia (triglycerides, cholesterol)
Options for Weight Loss • Self-directed Diet and exercise • Commercial Programs • Weight Watchers, Jenny Craig, NutriSystem • Usually 1200-1600cal/day • Traditional reduced calorie food regimen • Medically-supervised Very low or Low calorie diet (VLCD) • <800 cal/day • Incorporate meal replacements • Bariatric Surgery
Decision-Free VLCD/LCD (medically supervised) HMR Meal Replacements only: HMR Shakes, Cereal & Entrees Meal Replacements Shakes/Cereal + Entrees + Vegetables & Fruits HMR Structured Diet Boxes More structure. Fewer choices. More weight loss. No Decisions 60lbs Minimum Decisions 37lbs Phase 2: Management Grocery store food + Vegetables & Fruits + Meal Replacements Phone support
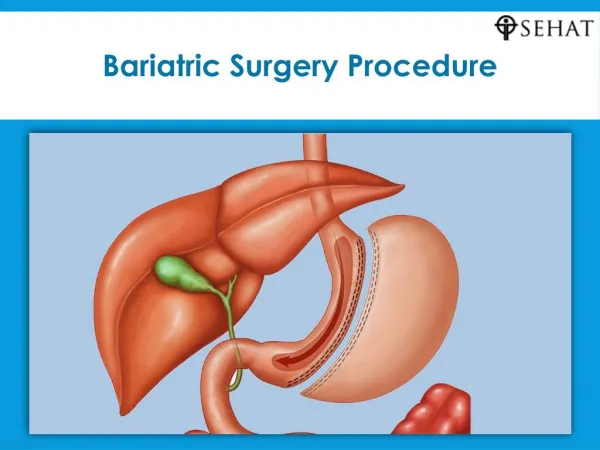
Surgery for Morbid Obesity • Historical • Jejuno-ileal bypass • Vertical banded gastroplasty • Biliopancreatic diversion • Duodenal Switch • Current • Roux-en-Y gastric bypass • Adjustable gastric banding • Sleeve gastrectomy Laparoscopic
Why Bariatric Surgery? • Improve health conditions associated with obesity • Improve quality-of-life • Prevent premature death associated with obesity • Likelihood of accompllishing this once >100lbs over ideal… vanishingly small.
Indications for Surgical Treatment • At least 5 years history of severe obesity • Multiple failed attempts at nonsurgical means of weight loss • BMI >40 kg/m2 or BMI >35 kg/m2 with associated with significant comorbidities (ie HTN, sleep apnea, diabetes, pseudotumorcerebri, etc.) • FDA: band: BMI >35 kg/m2 or BMI >30 kg/m2 with co-morbidities 1991 NIH Consensus Development Conference
Preoperative Assessment(Bariatric Surgical Team) • Nutritionist • Nurse practitioner/ Social worker • Psychiatrist • Internist/Cardiologist • Surgeon • Anesthesiologist
Patient Preparation • Risks/benefits of the procedure • Possible conversion • Nutritional sequelae • Need for long-term follow-up • Assess for obesity-related comorbidities • Change in lifestyle • Post-operative changes
Postoperative Management • Extubated in OR • Transferred to surgical ward • Nasogastric tube is not routinely used • Patient-controlled analgesia • Early ambulation • Incentive spirometry and deep breathing exercise • Contrast study on postoperative day 1 or 2