Download
1 / 21
210 likes | 431 Views
A DECISION SUPPORT SYSTEM ON SUTURE SELECTION. A . Erol Fazlıoğlu. History of the Suture.

E N D
A DECISION SUPPORT SYSTEM ON SUTURE SELECTION • A. Erol Fazlıoğlu
History of the Suture • The evolution of suturing material has brought us to a point of refinement that includes sutures designed for specific surgical procedures. They not only eliminate some of the difficulties the surgeon may have previously encountered during closure but decrease the potential for infection postoperatively. • Despite the sophistication of today's suture materials and surgical techniques, closing a wound still involves the same basic procedure used by physicians to the Roman emperors. The surgeon still uses a surgical needle to pull the suture strand as it is placed in tissue.
Personal Suture Preference-1 • Most surgeons have a basic "suture routine," a preference for using the same material(s) unless circumstances dictate otherwise. • The surgeon acquires skill, proficiency, and speed in handling by using one suture material repeatedly -- and may choose the same material throughout his or her entire career. A number of factors may influence the surgeon's choice: • his or her area of specialization. • operating room experience in medical school and resident training. • professional experience in the operating room. • knowledge of the healing characteristics of tissues and organs. • knowledge of the physical and biological characteristics of various suture materials. • patient factors (age, weight, overall health status, and the presence of infection).
Personal Suture Preference-2 • The surgeon's area of specialization plays a primary role in determining suture preference. • For example, obstetrician/gynecologists frequently prefer Coated Vicryl sutures for all tissue layers except, possibly, skin. • Most orthopaedic surgeons use Coated Vicryl sutures, PDS II sutures, and Stainless steel sutures. • Many plastic surgeons prefer ETHILON* nylon, Vicryl sutures or Monocryl sutures. • Most neurosurgeons prefer PERMA-HAND* Silk suture or Nurolon braided nylon suture. But no single suture material is used by every surgeon who practices within a specialty. • The surgeon's knowledge of the physical characteristics of suture material is also key. As the requirements for wound support vary with patient factors, the nature of the procedure, and the type of tissue involved, the surgeon will select suture material that will retain its strength until the wound heals sufficiently to withstand stress on its own. • The nature of suture material may elicit biological responses during the first post-operative week. While most suture materials will cause a mild reaction, synthetic materials tend to be less reactive than natural fibers. In addition, some suture materials become more inert -- or less reactive -- than others in the later phases of healing.
Suture Characteristics-1 If an ideal suture material could be created, it would be: • All-purpose, composed of material which could be used in any surgical procedure (the only variables being size and tensile strength). • Sterile. • Non-electrolytic, non-capillary, non-allergenic, and non-carcinogenic. • Non-ferromagnetic, as is the case with stainless steel. • Easy to handle. • Minimally reactive in tissue and not predisposed to bacterial growth. • Capable of holding securely when knotted without fraying or cutting. • Resistant to shrinking in tissues. • Absorbed with minimal tissue reaction after serving its purpose.
Suture Characteristics-2 However, because the ideal all-purpose suture does not yetexist, the surgeon must select a suture that is at least as close to the ideal as possible and maintain the following suture qualities: • High uniform tensile strength, permitting use of finer sizes. • Consistent uniform diameter. • Sterile. • Pliable for ease of handling and knot security. • Freedom from irritating substances or impurities for optimum tissue acceptance. • Predictable performance.
Suture Characteristics at a Glance • Size • Knot tensile strength • Monofilament vs. Multifilament Strands • Absorbable vs. Nonabsorbable Materials
SPECIFIC SUTURING MATERIALS Alphabetical Index • Chromic gut • Coated Vicryl • Ethibond • Gut, Chromic • Gut, Plain • Mersilene • Monocryl • Nurolon • PDS II • Plain Gut • Polydioxanone • Prolene • Silk Surgical • Surgical stainless steel • Surgical silk • Uncoated Vicryl • Vicryl • Vicryl, Coated • Vicryl, Uncoated
The Role of Sutures in Wound Healing • Impact of medical errors on patient safety • Joint Commission's new patient safety standards • To understand the integration process and how it affects infection control and patient safety • To prevent post-op wound infections
Principles Of Suture Selection-1 • Among the many decisions that face the surgeon in the operating room, suture selection for the procedure at hand may be one of the most critical. • Personal preference will, of course, play a role. But the final choice will depend upon various patient factors that influence the healing process, the characteristics of the tissues involved, and potential postoperative complications. • The wide variety of suturing materials available can make it difficult to choose the most appropriate suture for a given task.
Principles Of Suture Selection-2 When a wound reaches maximal strength, sutures are no longer needed. Therefore: • Close slow-healing tissues (skin, fascia, tendons) with nonabsorbable sutures or a long-lasting absorbable suture. • Close fast-healing tissues (stomach, colon, bladder) with absorbable sutures. • Foreign bodies in potentially contaminated tissues may convert contamination into infection. Therefore: • Avoid multifilament sutures which may convert a contaminated wound into an infected one. • Use monofilament sutures or absorbable sutures which resist harboring infection. Where cosmetic results are important, close and prolonged apposition of tissues and avoidance of irritants will produce the best results. Therefore: • Use the smallest inert monofilament suture materials (nylon, polypropylene). • Avoid using skin sutures alone. Close subcuticularly whenever possible. • Use sterile skin closure strips to secure close apposition of skin edges when circumstance permits. Foreign bodies in the presence of fluids containing high crystalloid concentrations may cause precipitation and stone formation. Therefore: • Use absorbable sutures in the urinary and biliary tracts. • Regarding suture size: • Use the finest size suture commensurate with the natural strength of the tissue to be sutured. • Use retention sutures to reinforce appropriately sized primary sutures if the patient is at risk of producing sudden strains on the suture line postoperatively. Remove the retention sutures as soon as that risk is reduced.
Material Selection?? All engineering designs require, atsomepoint, theselection ofmaterials and processes to shapethem. Development of asoftware tool, the CambridgeEngineering Selector (CES).
What others did? • Complete guide of suture selection depending on the procedure or the tissue involved. • Listed by types of surgery/tissue or by alphabetical order for easy access. • No HoN subscription but prepared by MD,PhD staff, a commercial tool.
What we did? (Here in Turkey) • A couple of booklets(translations) which imply material selection very roughly, prepared by ministry of health.
Climate for Change • Consumer activism • Increasing use of the Web by patients • The role of IT in support of quality healthcare • Organizational aspects of IT a critical success factor President’s Information Technology Advisory Committee (Healthcare report, February 2001)
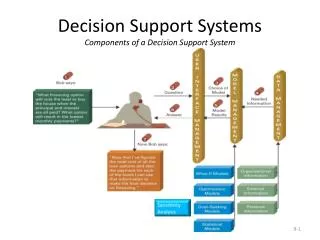
The Role of Computers in Decision Support • A clinical decision-support system is any computer program designed to help health professionals make clinical decisions. In a sense, any computer system that deals with clinical data or medical knowledge is intended to provide decision support. It is accordingly useful to consider three types of decision-support functions, ranging from generalized to patient specific.
Goals • It is clear that there is a need to make an improvement on patient safety(Proposals by FDA such as 21 CFR Part 878, Docket No. 02N-0288). • Using information technologies in order to obtain widely accepted suture selection standarts. • One more step in IT is to create a decision supportive mentor agent. • To be the assistant of health-care staff. • Initiatives of computer aided decision making in healthcare(2010+ Mentor Era).
Our Approach • We have to get most out of benefits of information technologies & communication. • Collecting Suture Selection Methods from literature and putting into a database • A Web based decision support tool on the net. • A Good project proposal for FP6(1st priority Biomedical Sciences, 2nd ly Information Tech.)
Partners & Resources • Dr. Sertaç Sever, Dermatology Clinic, Haydarpasa Numune Hospital. • http://scholar.google.com
Thanks for your attention! • Any questions? • A. Erol Fazlıoğlu