Download
1 / 26
290 likes | 743 Views
Interventional angiography. Initial success rates for patients with acute peptic ulcer bleeding are between 52 -98 % , with recurrent bleeding rates of 10 - 20 % Surgery and angio are equally effective following failed therapeutic endoscopy

E N D
Interventional angiography • Initial success rates for patients with acute peptic ulcer bleeding are between 52 -98 %, with recurrent bleeding rates of 10 - 20 % • Surgery and angio are equally effective following failed therapeutic endoscopy • Should be considered particularly in patients at high risk for surgery • Less likely to be successful in patients with impaired coagulation
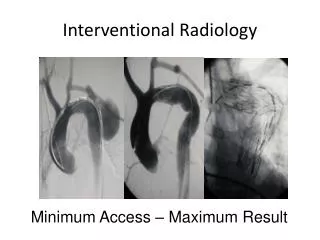
Urgent angiography of the left gastric artery revealed extravasation of contrast material from the gastric body
Successful arterial coil embolization, using super selective catheterization in the distal and proximal parts of the ruptured vessel
Indications for interventional angiography) American College of Radiology ( • Endoscopy is the best initial diagnostic and therapeutic procedure • Surgery and transcatheter arteriography are equally effective following failed therapeutic endoscopy • But transcatheter arteriography should be considered particularly in patients at high risk for surgery • Transcatheterarteriography is less likely to be successful in patients with impaired coagulation • Transcatheterarteriography is the best technique for treatment of bleeding into the biliary tree or pancreatic duct
Surgery is a reasonable alternative • TAE is not available • The lesion is deemed unlikely to respond to angiographic therapy • Underlying conditions that may complicate the ability to perform angiography or TAE (eg, renal insufficiency)
Angiovs surgery • 3271 patients with peptic ulcer bleeding • 88 patients (2.7 %) failed to have their bleeding controlled endoscopically. • 32 patients -underwent angiography • 56 -underwent surgery. • TAE was attempted in 26 patients and was successful in 23 of 26 patients (89 %). • Bleeding recurred -in 11 of 32 patients in the angiography group (34 %) v’s 7 of 56 (13 %) patients who underwent surgery • More complications were seen in the surgery group (68 versus 41 %). • The groups were similar with regard to 30-day mortality, length of hospital stay, and need for transfusion.
Indications for surgery for peptic ulcer hemorrhage • Failure of endoscopic therapy • Hemodynamic instability despite vigorous resuscitation (more than a 3 unit transfusion) • Shock associated with recurrent hemorrhage • Perforation
Secondary or relative indications • rare blood type • difficult crossmatch • refusal of transfusion • shock on presentation • advanced age • severe comorbid disease • chronic gastric ulcer as the origin of hemorrhage • elderly patients who are unlikely to tolerate prolonged attempts at resuscitation, large volume transfusions, or periods of hypotension
Emergently, surgery is associated with high mortality rates (up to 36 %) Early elective surgery is associated with a much lower mortality rate (0 - 7 %). Recurrent bleeding rates following surgery vary from 3- 23 %
Surgical Management • 10% of patients with bleeding ulcers still require surgical intervention for effective hemostasis. • The rate of bleeding PUD requiring surgical intervention has remained stable • Clinical and endoscopic parameters: • Shock and a low hemoglobin level at presentation • Forrest classification • The location and size of the ulcer
Doudenal ulcer • Expose ulcer with duodenotomy or duodenopyloromyotomy • Direct suture ligation, four quadrent ligation, ligation of gastroduodenal artery • Anti-secretory procedure • Truncal, parietal cell vagotomy • If unstable can use meds
Gastric ulcer • 10% are maliganant • 30% will rebleed with simple ligation • Need Resection • Distal gastrectomy with Bilroth I or II • Subtotal gastrectomy for 10% high on lesser curve
Tips • 5% to 10% of patients will have persistent bleeding that requires surgical intervention. • The vessel most likely to be bleeding is the gastroduodenal artery because of erosion from a posterior ulcer. • The duodenum is opened longitudinally, with the incision carried across the pylorus. • The vessel is oversewn, with a three-point U stitch technique, which effectively ligates the main vessel along with any smaller branches. • One must be careful to avoid incorporating the common bile duct into the stitch. • The duodenotomy is closed transversely to avoid narrowing
For type I gastric ulcers, even with appropriate preoperative evaluation, malignancy remains a major concern, and excision of the ulcer is necessary • types II and III gastric ulcers are associated with increased gastric acid levels, surgery for intractable disease should focus on acid reduction