Download
1 / 38
580 likes | 1.86k Views
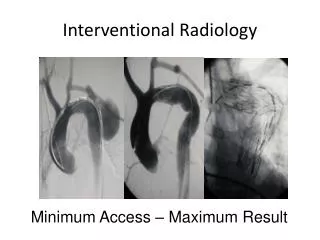
Interventional Oncology. Michael Kotton MD October 27, 2012. Objective. Understand role of thermal ablation in treatment of HCC Understand role of TACE in treatment of HCC Know patient selection criteria and possible complications of TACE and thermal ablation. Liver Cancer.

E N D
Interventional Oncology Michael Kotton MD October 27, 2012
Objective • Understand role of thermal ablation in treatment of HCC • Understand role of TACE in treatment of HCC • Know patient selection criteria and possible complications of TACE and thermal ablation
Liver Cancer • 5th most common cancer • 80% Hepatocellular Carcinoma (HCC) • 18,910 deaths in USA 2010 • Incidence increasing 4.3% per year • Underlying chronic liver disease/cirrhosis
Hepatocellular Carcinoma • Tends to stay localized to Liver • Can be cured by liver transplant • Prognosis depends on both cancer and underlying liver disease • Liver has a dual blood supply • Tumor supplied by hepatic artery
Interventional Options • Percutaneous • Thermal ablation, Chemical ablation • Transarterial • Bland embolization • Radioembolization • Chemoembolization • Drug Eluding Beads
How Do We Decide • Extent of Tumor • Milan Criteria (5/3 Rule) • One tumor less then 5 cm • Up to 3 tumors less then 3cm • No vascular invasion • Health of Patient • Condition of the Liver
Thermal Ablation • Curative Intent • Recurrence at 5 years 60-70% • Size <5cm • Solitary • Safe location • Not surgical candidate
Case 1 • 58 year old female • 2.2 cm tumor • Hep B • HTN • Normal Bilirubin • Mild PVH
Needle Placement RFA Probe Stomach
Post Treatment Pre Post
Complications • Bleeding • Infection • Tumor Seeding 2-10% • Subcapsular location • Inadvertent Ablation • Bowl, Gallbladder, Diaphragm • Central Biliary Tree
Outcome • <1% Mortality • Complications 5% • 30-55% five year survival • Local Recurrence 2-10% • Can be treated again • Recurrence at 5 years same as resection
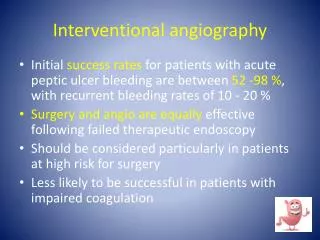
Chemoembolization • Large or multifocal tumors • Can Liver Tolerate Treatment • Patient benefit • Size and number of tumors
Patient Selection • Bilirubin < 3 • Albumin >3 • PLT >90 • No encephalopathy • No vascular Invasion • No Biliary Dilation • Tumor Less then 50% liver
Case 2 • 69 year old male • Hep B • 9 cm tumor • Normal Bilirubin • Mild PVH
Post Treatment Chung W et al. AJR 2012;199:349-359 Mannelli L et al. AJR 2009;193:1044-1052
Complications • Bleeding • Liver Failure • Infection • Biliary-Enteric Anastomosis • Post Embolization Syndrome • Fever, nausea, pain • Ends after 7 days, infection usually presents later • Inadvertent Embolization • Gallbladder, bowl
Does It Work • Survival Benefit in select patients • Hong Kong trial • 2 Year Survival 31% versus 11% • 3 Year Survival 26% versus 3% • Barcelona trial • 2 Year Survival 63% versus 27%
Summary • Remember the 5/3 rule • Transplantation is best treatment in eligible patients • Ablation for small tumors and resection for non cirrhotic livers • Chemoembolization for non surgical tumors who can tolerate the procedure
Case 3 • 68 year old female • Hep C • Multifocal tumors (5.2cm,3cm,2cm) • Good liver function
RESPONSE 2
Case 4 • 79 male • Hep C Cirrhosis • 3.7 cm solitary tumor • Multiple medical problems
Case 5 • 62 year old female • Hep C • Cirrhosis • 2.4 cm tumor • Otherwise healthy