Download
1 / 46
460 likes | 477 Views
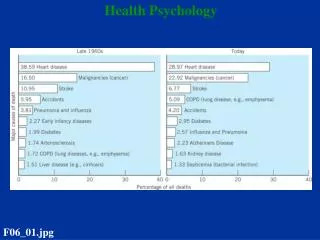
This keynote address discusses the problem of non-adherence to medical and psychological treatments, explores the causes of non-adherence, and highlights the role of health psychology in developing interventions to improve treatment adherence.

E N D
TAKING THE TREATMENT How can Health Psychology help? John Weinman Health Psychology Section Psychology Dept. (at Guy’s) IOP, Kings College London Keynote address at NZ Psychology Society & NZCCP Conference 20-23 April 2012
“ Drugs don't work in patients who don't take them “ ( C. Everett Koop, M.D. US Surgeon General , 1981-9 )
ADHERENCE / COMPLIANCE The extent to which patients follow medical treatment and advice • RESEARCH focuses on :- • the nature, patterning and levels of adherence • factors which explain / predict non-adherence • development / evaluation of interventions
The problem of non-adherence WHO report on non-adherence • Estimated that over 30 -50% medicines prescribed for long term illnesses are not taken as directed • Similar levels for psychol treatments - e.g . Attendance/homework for CBT • If treatment is evidence- based, then this represents a loss for patients and for the health care system
Risk of hospitalisation & non-adherence Sokol MC, McGuigan KA, Verbrugge RR, Epstein RS. Impact of medication adherence on hospitalization risk and healthcare cost. Medical Care. 2005;43:521-530.
CAUSES OF NON-ADHERENCE • Common myths • Current evidence
Myth 1: Non-adherence is a feature of the disease Non-adherence is not linked to type of disease Low adherence rates are problematic in most chronic diseases e.g. • HIV1 • Cancer2 • Heart disease3 • Rheum. arthritis4 • Diabetes5 • Asthma6 4Hill et al. Ann Rheum Dis 2001; 869-875. 5Glasgow et al. J Behav Med 1986;9:65–77. 6Cochrane et al. Respir Med 1999;93:763–769.. 1Friedland, Williams. AIDS 1999;13(Suppl 1):S61–72. 2Lilleyman, Lennard. BMJ 1996;313:1219–1220. 3Horwitz et al. Lancet 1990;336:1002–1003.
Myth 2 • Non-adherence is related to: • Gender • Educational experience • Intelligence • Marital status • Occupation / income • Ethnic background
Adherence Rates Vary Between patients Within the same patient over time and across treatments Most patients will be non-adherent some of the time
Myth 3 • Non-adherence is easily fixed by : - • Providing information • Providing reminders • Being authoritative • Fear arousal
ADHERENCE INTERVENTIONS Cochrane review: Haynes et al (2008) “Current methods of improving adherence are mostly complex and not very effective, so that the full benefits of treatment cannot be realized. High priority should be given to fundamental and applied research concerning innovations to assist patients to follow medication prescriptions for long-term disorders”
How can Health Psychology help? Need to understand types and causes of non-adherence Need to tailor interventions to take account of this Develop & test theoretical models
UNINTENTIONAL NON-ADHERENCE • RANGE OF POSSIBLE FACTORS :- • Poor HCP-Patient Communication • Low patient satisfaction and/or recall • Problems in planning/executive function • or prospective memory • Financial or other barriers
Beliefs influence unintentional non-adherence - forgetfulness2 1 BCG Harris 2002; Conrad Soc Sci Med 1985;20:29–37; Ley 1988; Peterson Am J Health-Syst Ph 2003;60:657–65 2 Unni , Pat Edu Coun 2010 doi:10.1016/j.pec.2010.05.006
INTENTIONAL NON-ADHERENCE • Patients know what to do & how to do it • BUT are reluctant to adhere because either :- • TREATMENT DOESN’T MAKE SENSE • WORRIES/CONCERNS ABOUT TREATMENT
What are the key beliefs influencing adherence to treatment? Patients’ perceptions of illness Patients’ perceptions of treatment
Core beliefs about Illness • IDENTITY Abstract label eg, hypertension; asthma; arthritis • Concrete symptoms that a person associates with the condition • CAUSAL BELIEFS Stress, environment, genetics, own behaviour, ageing etc • TIMELINE Perceived duration and profile eg, chronic, acute, cyclical • CONSEQUENCES Personal, economic, social • CURE / CONTROL Beliefs about the amenability to control or cure
ILLNESS PERCEPTION & treatment adherence • Some illness perceptions are associated with treatment adherence in some conditions :- e.g. - causal beliefs predict adherence behaviour in post- MI (Weinman et al, 2000) - timeline beliefs predict preventer medication adherence in asthma (Horne, Weinman, 2002) - causal, timeline & control beliefs predict adherence to CBT for Psychosis (Freeman et al, in press) • BUT – illness beliefs per se are not strong predictors of treatment adherence – need to consider more proximal predictors (ie patients’ beliefs re. treatment)
Illness Treatment
GOODNESS OF FITbetween illness reps and treatment recommendations • Patients evaluate the need for treatment in the light of their understanding of illness • But some treatments may not make sense :- - exercises for back pain , balance disorder etc - daily adherence to preventer medication in asthma - smoking cessation in early cervical cancer - phosphate binding medication in ESRD • CHALLENGE TO HP – to identify these situations and to assess treatment beliefs -- develop interventions to increase adherence goodness of fit and increase motivation to adhere
TREATMENT BELIEFS: What is the patient's perspective ?
Beliefs about Medicines Questionnaire (BMQ) SPECIFIC BELIEFS about medicines prescribed for a particular illness GENERAL BELIEFS about medicines as a whole
SPECIFIC BELIEFS Views about prescribed medication Necessity Beliefs about necessity of prescribed medication for maintaining health Concerns Arising from beliefs about potential negative effects
Studies in asthma, CHD, cancer, renal dialysis, HIV/Aids, hypertension, diabetes Horne et al (in press), Cooper et al (2002), Horne et al (2001), Horne & Weinman (2002), Horne (2000), Horne & Weinman (1999) Horne et al (1999), Horne (1988) Low adherence Doubts about NECESSITY CONCERNS about potential adverse effects
SUMMARY Patients’ beliefs about their illness and treatment • Influence adherence • Have an internal logic • Are influenced by symptoms • May differ from the ‘medical view’ • May be based on mistaken beliefs/premises • May not be disclosed in consultation • Are not set in stone and can be changed
Implications for health care ? • Use the consultation to anticipate and plan • Interventions to :- • - improve goodness of fit • - improve understanding of illness and treatment
Using the consultation to facilitate informed adherence • Check patient’s understanding of treatment and , if necessary :- • Provide clear rationale for NECESSITYof treatment • Elicit and address CONCERNS • Agree practical plan for how,where and when to take treatment • Identify any possible barriers NEEDS TRAINING OF HCPs – studies in progress
Interventions to improve adherence • Now a number of successful approaches which • are based on a good understanding of patients’ beliefs, • using different media, such as :- • text messaging • web-based interactive programmes • phone based support
Improving adherence :The example ofPreventer medication in asthma
Asthma & patient self management • Common, chronic condition • Caused by inflammation of the airways • Characteristic symptoms include • Tightness in chest • Shortness of breath • Wheezing • Cough • Patient prescribed reliever medication & preventer medication
Non-adherence to asthma preventer medication • Non-adherence common • Adherence rates of between 10-50% frequently reported • Non-adherence costly • Increase in symptoms • Increase in healthcare utilisation • Reduction in quality of life • Reasons for non-adherence vary • Patient beliefs among factors most consistently associated with non-adherence to preventer medication • Beliefs about illness • Beliefs about medication
Relationships between illness and medication beliefs and self-reported adherence
Patient beliefs associated with non-adherence • Beliefs about illness • BIPQ (Broadbent, Petrie, Main & Weinman, 2006) • Low/high Identity • Short or episodic Timeline • Low/high Consequences • Low Coherence • Low Cure/Control • Beliefs about medication • BMQ (Horne, Weinman & Hankins, 1999) • Low Necessity • High Concerns
Profiling patients based on risk of non-adherence Non-Adherent profile Adherent profile Timeline Personal control Treatment control Identity Consequences Medication necessity Medication concerns 0 10 20 30 40 50 60 70 80 90 100
British Journal of Health Psychology Volume 17, Issue 1, pages 74–84, February 2012
Baseline assessment Adherence assessments at 6,12, 18 weeks and 6 months 212 patients aged 16-45 recruited from medicine package inserts or heath websites - dx asthma (not COPD), not taking preventer meds as prescribed Normal care Method Tailored Txt messages 18 weeks
Your preventer controls your asthma over the long term & stops attacks Targeted Texting Timeline Personalcontrol Treatment control Illness consequences Your asthma is always there, even when you don’t have symptoms Your preventer is safe to take every day Medication necessity Medication concerns
Preventer Adherence Levels Mean compliance score Compliance = puffs taken/puffs prescribed Group difference p <.01
Percentage of patients reporting adherence at 80% or greater in control and intervention groups
Conclusions • A better understanding of patients perspectives of illness and treatment is key to understanding adherence • This approach offers a simple framework for identifying and addressing the key barriers to adherence to medication • Urgent need to develop coherent theory & theory-based interventions