Download
1 / 21
210 likes | 376 Views
BUDGETING FOR HIV/AIDS - Costing the ‘Indirect Impact’ on the Health Sector. Namibia, Aug 2003. Teresa Guthrie Research Unit on AIDS & Public Finance Budget Information Service. Measuring the ‘Indirect Impact’ of HIV/AIDS on the Health System.

E N D
BUDGETING FOR HIV/AIDS - Costing the ‘Indirect Impact’ on the Health Sector Namibia, Aug 2003. Teresa Guthrie Research Unit on AIDS & Public Finance Budget Information Service
Measuring the ‘Indirect Impact’ of HIV/AIDS on the Health System The HIV/AIDS pandemic has become the greatest challenge not only to health in Southern Africa, but to development in general. Various socio-economic impact studies have been done, projections of costs of specific HIV interventions (prevention, treatment, support etc.), public, private & personal costs Research Unit on AIDS and Public Finance ~ Idasa ~ 12 Aug 2003
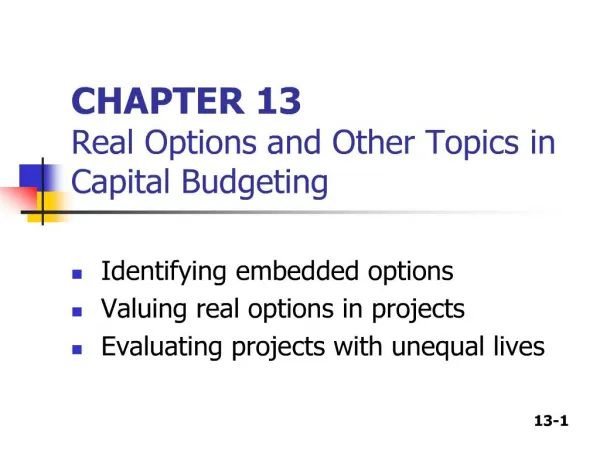
Indirect expenditureas result of impactof HIV/AIDSe.g. increased demand for social security grants, higher hospital bed occupancy, medicine for OIs Direct expenditureon HIV/AIDS programmese.g. condoms, PMTCT, public awareness campaigns On recurrent or operation budget (State Revenue Fund) On development budget (partially covered by donors) Usually requires unconditional transfers or general budget support Best addressed using earmarked/ring-fenced funds
Quantifying those ‘indirect costs’... • That is, the extra ‘burden’ on existing health services due to the increased demand for treatment and care of OIs, LRTIs, TB, STDs etc • More difficult to quantify the less direct costs and losses, to individuals, families, communities and the state. • How much should govt. allocate to enable the over-stretched health services to continue ot provide quality care? Research Unit on AIDS and Public Finance ~ Idasa ~ 12 Aug 2003
Challenges of Costing the Indirect Impact Notifiability and Identification • HIV infection is not a notifiable disease in many African countries. • Many countries do not conduct routine voluntary HIV testing on patients. • Confidentiality of HIV status must be respected • Thus, it is almost impossible to identify HIV+ patients attending health facilities, to quantify the cost of their services and to compare these costs with those of HIV- patients.
Challenges of Costing the Indirect Impact (2) Stages of the Syndrome • HIV infection presents as a syndrome of many infections, illnesses. • In the earlier stages of the illness, OIs, STDs, TB are common, but cannot be directly attributed to HIV without test results. • Thus surveillance usually only captures patients once they reach stage 3 or 4 of the illness, when more symptomatic. • At same time, mainstreaming efforts would not wish to distinguish HIV-specific services from non-HIV.
Challenges of Costing the Indirect Impact (3) Varying costs • Obviously the costs in the later stages are greater than in the earlier stages. • But costs of earlier stages difficult to separate from general health service costs - little info. • Many studies use these infections as ‘proxies’ to identify HIV+ patients - this is not ideal/accurate. Research Unit on AIDS and Public Finance ~ Idasa ~ 12 Aug 2003
Challenges of Costing the Indirect Impact (4) Data Limitations • Inaccuracies of prevalence data/ projections - can’t accurately calculate how many people are currently infected and at which stage, can’t quantify and cost their need for services. • Limited availability, quality, validity & reliability of data on which to base costings. • Lack of sophisticated information systems and trained personnel to use them. • Even less data at district level, where the services are delivered and the greatest impact felt…. Research Unit on AIDS and Public Finance ~ Idasa ~ 12 Aug 2003
Limitations of Existing ‘Indirect’ Costing Studies • Many studies use ‘proxies’ forf HIV status. • Most single studies (‘snap-shot’ vs longitudinal), over a short specific time - therefore do not capture the frequency of visits as patient becomes more ill. • Usually single site, problematic to extrapolate to national costs. • Most limited to financial costs to the service-provider, do not measure economic impact to all role-players, such as costs to family (financial, time, energy etc).
Other considerations... • The background burden and demand for services (non-HIV related) remains. • Increasing HIV+ patients at health facilities may decrease the access for patients with other chronic conditions. • Rationing - anecdotal evidence that HIV+ patients are being turned away from health services, due to high demand for services and a sense of not being able to ‘do anything’. Research Unit on AIDS and Public Finance ~ Idasa ~ 12 Aug 2003
Importance of Estimating the Indirect Costs…. • In order to allocate sufficient funds to service-delivery, for infra-structural and capacity development to accommodate the greater demand due to HIV. • “The important message is that there is still much to be done to help policy makers plan and manage this epidemic so that it has as minimal impact as possible on the health system” (Franklin, Desmond, Manning, 2001) Research Unit on AIDS and Public Finance ~ Idasa ~ 12 Aug 2003
Overview of Available Literature • Few African studies. • Some infection-specific costings eg. TB (but can’t assume that all are HIV-related). • No. of visits, length of stay, cost per visit (vs non-HIV), bed occupancy, no. of admissions. • Costs to families (some looking at funeral costs). • Level of service differences, rural/urban differences. • Little/ none out-patient care/ primary health care. • Some HBC costs but not compared to hospital costs. • Little on child health needs and costs.
Country Studies Refer to Article
Namibia Inpatient Services Research Unit on AIDS and Public Finance ~ Idasa ~ 12 Aug 2003
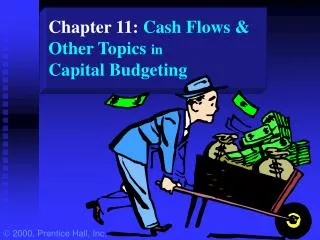
Burkino Faso: Impacts of HIV/AIDS on the Health-Care Sector for Various Scenarios ** As a percentage of the 1999 budget. Source: Boily, Larivière, Martin at the IDEA International Institute
TANZANIA : Recurrent and development health expenditure Research Unit on AIDS and Public Finance ~ Idasa ~ 12 Aug 2003
South Africa: Estimates of public health (indirect) expenditure on HIV/AIDS • DOH estimates very significant expenditure incurred by public health system: Combined national and provincial expenditure on HIV/AIDS = R4.4448 bn or 15.0% of 2001/2 consolidated public health expenditure • In 2000, estimated 628 000 admissions to public hospitals for AIDS-related illnesses, or 24% of all public hospital admissions (DoH, Abt) • Cost of hospitalising AIDS patients (public facilities) = R3.6 billion in 2001/2 = 12.5% of total public health budget
Recommendations (1) • Improve systems : • data collection and information management • budgeting and planning • accounting and tracking • capacity building to manage these systems Research Unit on AIDS and Public Finance ~ Idasa ~ 12 Aug 2003
Recommendations (2) • Public Health Facilities Improvement: • Allocate funds to improve services for the prevention and treatment of OIs, TBs, STDs, RTIs, diarrhoea, etc. • Funds for general improvement of health services, personnel, infrastructural development etc • Funds for ‘step-down’ facilities for last stages of illness Research Unit on AIDS and Public Finance ~ Idasa ~ 12 Aug 2003
Recommendations (3) • Funding Mechanisms • Conditional grants to ensure delivery of specific programmes • Non-conditional transfers to regions for general improvement of health services • Co-ordination of donor funds Research Unit on AIDS and Public Finance ~ Idasa ~ 12 Aug 2003
Thank you For more information, contact: Teresa Guthrie Research Unit on AIDS & Public Finance, Budget Information Service Idasa teresa@idasact.org.za