Download
1 / 60
650 likes | 1.05k Views
COMMON DISEASES IN FAMILY PRACTICE. Department of Family and Community Medicine University of the Philippines-Philippine General Hospital. COMMON DISEASES. DYSPEPSIA URINARY TRACT INFECTION HYPERTENSION BRONCHIAL ASTHMA PULMONARY TUBERCULOSIS DIABETES MELLITUS. dyspepsia. DYSPEPSIA.

E N D
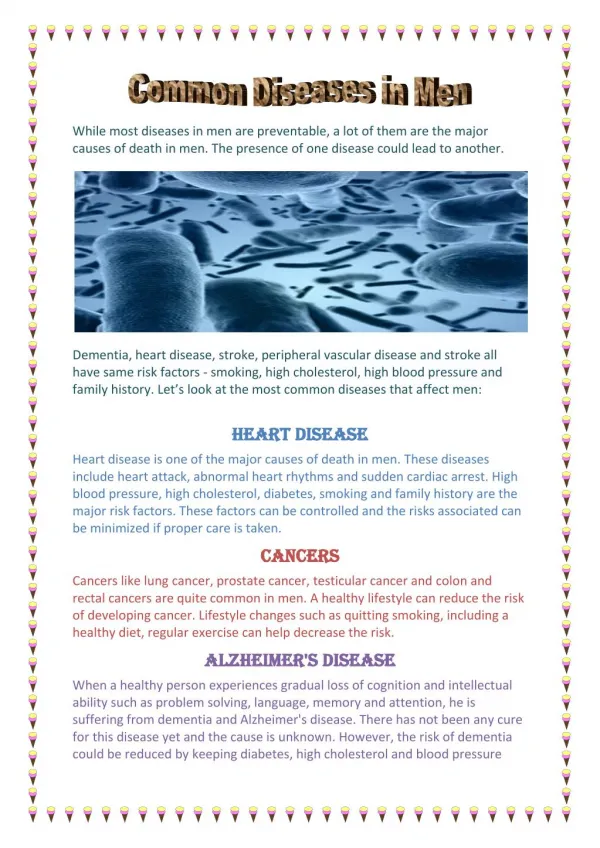
COMMON DISEASES IN FAMILY PRACTICE Department of Family and Community Medicine University of the Philippines-Philippine General Hospital
COMMON DISEASES • DYSPEPSIA • URINARY TRACT INFECTION • HYPERTENSION • BRONCHIAL ASTHMA • PULMONARY TUBERCULOSIS • DIABETES MELLITUS
DYSPEPSIA • bloatedness, fullness, gnawing or burning • epigastric area • continously or intermittently • more than 2 weeks • chronic or recurrent • associated with : anorexia, early satiety, belching, nausea, regurgitation, vomiting • with or without alarm symptoms/signs
Dyspepsia: alarm features 1. age at onset >45 2. weight loss 3. anemia 4. hematemesis 5. melena 6. hematochezia 7. dysphagia 8. odynophagia 9. persistent vomiting 10. abdominal mass 11. jaundice 12. chronic NSAID intake 13. chronic alcohol intake 14. previous history of ulcer
DYSPEPSIA Pharmacologic Treatment: 2-4 wks PPI Non-Pharmacologic Advice: avoid alcohol, milk, tea, carbonated drinks, coffee, acidic beverages, small frequent feedings, avoid skipping meals WOF: increased abdominal pain, alarm symptoms, absence of improvement after >7days of tx
Proton pump inhibitors • Esomeprazole 20 and 40mg OD • Omeprazole 20 and 40mg OD • Rabeprazole 20mg OD • Pantoprazole 40mg OD • Lansoprazole 15 and 30 mg OD
URINARY TRACT INFECTION • ACUTE UNCOMPLICATED CYSTITIS IN WOMEN • ACUTE UNCOMPLICATED PYELONEPHRITIS IN WOMEN • ASYMPTOMATIC BACTERIURIA IN ADULTS • UTI IN PREGNANCY • RECURRENT UTI IN WOMEN • COMPLICATED UTI • UTI IN MALES The Philippine Clinical Guidelines on the Diagnosis and Management of Urinary Tract Infections in Adults 2004
ACUTE UNCOMPLICATED CYSTITIS IN WOMEN • Dysuria, frequency or gross hematuria, with or without backpain • Without symptoms of vaginitis, pyelonephritis, risk factors for subacute pyelonephritis or complicated UTI • >100 CFU/mL; ≥5 wbc/hpf • Standard urine microscopy is not a prerequisite for treatment • Pre-treatment urine culture and sensitivity is not recommended
ACUTE UNCOMPLICATED PYELONEPHRITIS IN WOMEN • fever (>38C), chills, flank pain, CVA tenderness, nausea, vomiting ±lower UTI symptoms • >10,000 CFU/mL; >5 wbc/hpf • Urinalysis and gram stain are recommended • Urine culture and sensitivity should be performed routinely to facilitate cost-effective use of antibiotics • Non-pregnant patients with no signs and symptoms of sepsis, adherent to treatment and likely to return for follow-up may be treated as outpatients
ACUTE UNCOMPLICATED PYELONEPHRITIS IN WOMEN INDICATIONS for ADMISSION: • inability to maintain oral hydration or take medications • concern about compliance • uncertainty about the diagnosis • severe illness with high fever, severe pain, marked debility • signs of sepsis
ASYMPTOMATIC BACTERIURIA IN ADULTS • > 100,000 cfu/ml of one or more uropathogens in 2 consecutive midstream urine specimen or in one catheterized urine specimen in the absence of symptoms attributable to UTI • Screening: • who will undergo genitourinary manipulation or instrumentation • post-renal transplant patients up to the first six months • DM patients with poor glycemic control • ALL pregnant women
ASYMPTOMATIC BACTERIURIA IN ADULTS • Any antibiotics for AUC can be used for treatment of ASB in the above group of patients • 7-14 day course is recommended, except for pregnant women • Routine screening and treatment is not recommended for healthy adults • URINE CULTURE is the recommended screening test, but urine microscopy and stain may be used in the absence of culture
UTI IN PREGNANCY • > 100,000 cfu/ml of one or more uropathogens in 2 consecutive midstream urine specimen or in one catheterized urine specimen in the absence of symptoms attributable to UTI • Must be screened on their first prenatal visit between 9-17 wks AOG • URINE CULTURE of clean catch midstream urine is the test of choice
UTI IN PREGNANCY • Antibiotic treatment must be initiated upon diagnosis • Follow-up cultures one week after completing the course of treatment • Treatment - Nitrofurantoin (not for those near term) - Co-amoxiclav and cephalexin - Cotrimoxazole (not in the 1st and 3rd trimester) - 7-day course is recommended
RECURRENT UTI • Episodes of acute uncomplicated UTI documented by urine culture occurring >2x/yr in a non-pregnant woman without known urinary tract abnormality • Treatment of individual episodes: 7-day treatment • Prophylaxis (continuous and post-coital)
COMPLICATED UTI • significant bacteriuria is >100,000 cfu/ml • Urine sample for gram stain, culture and sensitivity testing pretreatment is a MUST • Recommendation for mild to moderate illness: oral fluoroquinolones for 7-14 days • A repeat urine culture after one to two weeks of therapy
UTI IN MALES • Generally considered complicated • However, the 1st episode of symptomatic LUTS occurring in young (15-40 years old) otherwise healthy sexually active men with no clinical or historical evidence of structural or functional urologic abnormality is considered uncomplicated UTI • Significant pyuria is >5wbc/hpf in a clean catch midstream urine specimen • TREATMENT: 7-day antibiotic regimen of TMP-SMZ or Fluoroquinolones may be used
HYPERTENSION • Diagnostic workup: - FBS - U/A - serum Crea - Serum K - Lipid profile (HDL,LDL, Chole, Trigly) - 12 L-ECG • Treat to BP < 140/90 or < 130/80 mmHg in patients with diabetes or chronic kidney diseases
HYPERTENSION HYPERTENSIVE URGENCY - no end organ damage - oral medications given initially - lower BP within 2-3 days HYPERTENSIVE EMERGENCY -(+) changes in sensorium, papilledema, or CHF - IV meds given STAT - lower BP within 24 hours
HYPERTENSION PO MEDICATIONS: 1. Calcibloc (Nifedipine) • 5-10 mg SL or PO, Q30 mins 2. Captopril (Capoten) • 25 mg SL or PO, Q30 mins 3. Clonidine ( Catapress) • 75 mcg SL or PO, Q1
ATS CLASSIFICATION 0 – No TB exposure 1 – TB exposure, No evidence of infection 2 – TB infection, No evidence of disease 3 – TB clinically active 4 - TB not clinically active 5 – TB suspect (diagnosis pending)
WHO CLASSIFICATION of PTB • Pulmonary Tuberculosis (PTB) • Smear positive - if at least two sputum specimens are AFB (+). • Smear negative - if none of the specimens are AFB (+). • Extrapulmonary tuberculosis (EPTB)
CATEGORIES of PTB NEW CASE: • A patient who has never had treatment for TB or, if with previous anti-TB medications, that was taken for less than four weeks. RELAPSE: • A patient who has been declared cured of any form of TB in the past by a physician after one full course of anti-TB medications, and now has become sputum smear (+)
CATEGORIES of PTB RETURN AFTER DEFAULT (RAD) • A patient who stops taking his medications for two months or more and comes back to the clinic smear (+). FAILURE • A patient who, while on treatment, remained or became smear (+) again at the fifth month of anti-TB treatment or later; or a patient who was smear (-) at the start of treatment and becomes smear (+) at the 2nd month.
CATEGORIES of PTB TRANSFER-IN • A patient whose management was started from another area and now transferred to a new clinic CHRONIC CASE • A patient who became or remained smear (+) after completing fully a supervised retreatment regimen
DIAGNOSIS of PTB • In the Philippines, cough of two weeks or more should make the physician and/or other healthcare workers suspect the possibility of pulmonary tuberculosis. [Grade A Recommendation] • Cough with or without the following: night sweats, weight loss, anorexia, unexplained fever and chills, chest pain, fatigue and body malaise, is suggestive of TB. • A patient exhibiting cough of two weeks or more with or without accompanying symptoms will be referred to as a TB Symptomatic
INITIAL WORK-UP • The initial work-up of choice for a TB symptomatic is the sputum microscopy. All patients who present with cough of two weeks or more should preferably have three, but at the least two sputum specimens sent for sputum microscopy for Acid Fast Bacilli (AFB). [Grade A Recommendation] • Sputum microscopy is still the most efficient way of identifying cases of tuberculosis.
INITIAL WORK-UP • Sputum smear for AFB is available, accessible, affordable, with results rapidly available, correlates well with infectiousness. • While there is new evidence that the third sputum specimen usually contributes minimally to the diagnosis of active tuberculosis, three sputum specimens are still recommended until the same findings are validated in the local setting. [Grade C Recommendation]
SPUTUM MICROSCOPY • Patients must be encouraged to bring up sputum and not saliva. • Sputum collected first thing in the morning for three consecutive days is recommended [Grade C Recommendation].
SPUTUM MICROSCOPY • Other modified schedules to allow collection in the shortest number of days and clinic visits is likewise acceptable [Grade C Recommendation]: Advise the patients to collect three sputum specimens within two days as follows: • First Specimen: Spot specimen collected at the time of first consultation • Second Specimen: Early morning specimen • Third Specimen: Second spot specimen collected when patient comes back the next day.
PULMONARY TUBERCULOSIS TREATMENT COMPLETED: • treatment completed but does not meet criteria to be classified as "cure" or "failure“ TREATMENT FAILURE: • AFB Sputum Smear (+) after five months of treatment OR AFB Sputum Smear (-) before treatment and becomes (+) during treatment
TREATMENT • The recommended treatment regimen for all adults newly diagnosed with smear-positive tuberculosis and no history of treatment is a short-course chemotherapy (SCC) regimen, consisting of two months of isoniazid, rifampicin, pyrazinamide and ethambutol (2HRZE) in the initial phase, and 4 months of isoniazid and rifampicin (4HR) in the continuation phase [Grade A]. • The initial phase of treatment (2HRZE) should be given daily, followed by daily or thrice-weekly administration of isoniazid and rifampicin during the continuation phase.