Download
1 / 37
400 likes | 782 Views
Pediatric Scoliosis OMT Module. American College of Osteopathic Pediatricians Robert Hostoffer, DO,FACOP, FAAP. edited by Eric Hegybeli, DO, FACOP. Background:.

E N D
Pediatric Scoliosis OMT Module • American College of Osteopathic Pediatricians • Robert Hostoffer, DO,FACOP, FAAP • edited by • Eric Hegybeli, DO, FACOP
Background: Andrew Taylor Still, was born in Virginia in 1828, the son of a Methodist minister and physician. At an early age, Still decided to follow in his father's footsteps as a physician. After studying medicine and serving an apprenticeship under his father, Still became a licensed M.D. in the state of Missouri. Later, in the early 1860's, he completed additional coursework at the College of Physicians and Surgeons in Kansas City, Missouri. He went on to serve as a surgeon in the Union Army during the Civil War.
Background: • After the Civil War and following the death of three of his children from spinal meningitis in 1864, Still concluded that the orthodox medical practices of his day were frequently ineffective, and sometimes harmful. He devoted the next ten years of his life to studying the human body and finding better ways to treat disease.
Background: His research and clinical observations led him to believe that the musculoskeletal system played a vital role in health and disease and that the body contained all of the elements needed to maintain health, if properly stimulated. Still believed that by correcting problems in the body's structure, through the use of manual techniques now known as osteopathic manipulative treatment, the body's ability to function and to heal itself could be greatly improved. He also promoted the idea of preventive medicine and endorsed the philosophy that physicians should focus on treating the whole patient, rather than just the disease. • http://www.aacom.org/OM/history.html
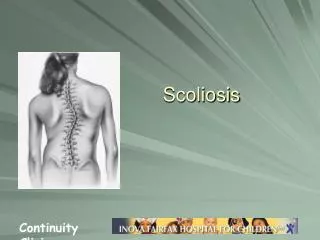
Classification of Scolosis • Nonstructural scoliosis • postural scoliosis • compensatory scoliosis
Transient Structural Scoliosis • sciatic scoliosis • hysterical scoliosis> • inflammatory scoliosis
Structural Scolosis • idiopathic (70 - 80 % of all cases) • congenital • neuromuscular • poliomyelitis • cerebral palsy • syringomyelia • muscular dystrophy • amyotonia congenita • Friedreich's ataxia • neurofibromatosis • mesenchymal disorders • Marfan's syndrome • Morquio's syndrome • rheumatoid arthritis • osteogenesis imperfecta • certain dwarves • trauma • fractures • irradiation • surgery
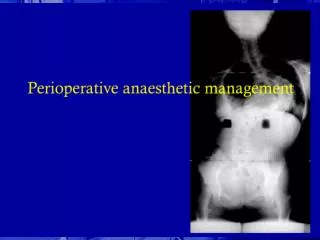
Osteopathic Considerations Type II (non-neutral) mechanics occur at the transitional areas between the spinal curves In scoliosis, flexed vertebral dysfunctions are typically found in the lumbar region; extended dysfunctions in the thoracic region Scoliosis usually is not secondary to a short leg
Osteopathic Considerations - Treatment *Infantile scoliosis can be treated fairly effectively by addressing the occiput (usually with cranial), cervicothoracic and sacroiliac areas *Treatment of older patients is focused on mobilizing restricted areas with OMT, stretching tightened tissues on the convex side, strengthening weak muscles on the concave side and correcting posture
Innervation Table Organ/System Parasympathetic Sympathetic Ant. Chapman's Post. Chapman's EENT Cr Nerves (III, VII, IX, X) T1-T4 T1-4, 2nd ICS Suboccipital Heart Vagus (CN X) T1-T4 T1-4 on L, T2-3 T3 sp process Respiratory Vagus (CN X) T2-T7 3rd & 4th ICS T3-5 sp process Esophagus Vagus (CN X) T2-T8 --- --- Foregut Vagus (CN X) T5-T9 (Greater Splanchnic) --- --- Stomach Vagus (CN X) T5-T9 (Greater Splanchnic) 5th-6th ICS on L T6-7 on L Liver Vagus (CN X) T5-T9 (Greater Splanchnic) Rib 5 on R T5-6 Gallbladder Vagus (CN X) T5-T9 (Greater Splanchnic) Rib 6 on R T6 Spleen Vagus (CN X) T5-T9 (Greater Splanchnic) Rib 7 on L T7 Pancreas Vagus (CN X) T5-T9 (Greater Splanchnic), T9-T12 (Lesser Splanchnic) Rib 7 on R T7 Midgut Vagus (CN X) Thoracic Splanchnics (Lesser) --- --- Small Intestine Vagus (CN X) T9-T11 (Lesser Splanchnic) Ribs 9-11 T8-10 Appendix T12 Tip of 12th Rib T11-12 on R Hindgut Pelvic Splanchnics (S2-4) Lumbar (Least) Splanchnics --- --- Ascending Colon Vagus (CN X) T9-T11 (Lesser Splanchnic) R Femur @ hip T10-11 Transverse Colon Vagus (CN X) T9-T11 (Lesser Splanchnic) Near Knees --- Descending Colon Pelvic Splanchnic (S2-4) Least Splanchnic L Femur @ hip T12-L2 Colon & Rectum Pelvic Splanchnics (S2-4) T8-L2 --- ---
Print out the answer sheet to use with the following questions.
Circle the correct answer and review with director: • Question1: A, B, C, D, E. • Question2: A, B, C, D, E. • Question3: A, B, C, D, E.
Question: • 1. Inflammatory Scoliosis is considered a: A. Transient scoliosis B. Structural C. Idiopathic D. Neurogenic E. NonStructural
2. All of the following are causes of structural scoliosis except: • Wedge vertabrae • Hemivertebrae • Congenital Bar • Block vertebra • Circular wedge
3. All are curves found in scoliosis except: A. Thoracic curve B Cervico/thoracic curve C. Lumbar curve D. Double major curve E. Thoraco/lumbar curve
Certificate of Completion • I, _________________________, successfully completed the Pediatric OMT Module on __ __ 20__ Signatures: • Pediatric Resident ____________________ • Pediatric Residency Director____________ • ( Please print and give to program director.)