Download
1 / 19
350 likes | 1.84k Views
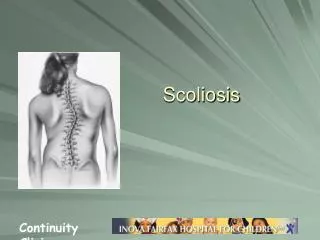
SCOLIOSIS. A condition that involves complex lateral and rotational curvature of the spine. Dextroscoliosis is a scoliosis with the convexity on the right side. Levoscoliosis is a scoliosis with the convexity on the left side. Medical ppt. http://hastaneciyiz.blogspot.com. Classification.

E N D
SCOLIOSIS A condition that involves complex lateral and rotational curvature of the spine. Dextroscoliosis is a scoliosis with the convexity on the right side. Levoscoliosis is a scoliosis with the convexity on the left side. Medical ppt http://hastaneciyiz.blogspot.com
Classification Postural Scoliosis The deformity is secondary or compensatory to some condition outside the spine; when the patient sits (thereby cancelling leg asymmetry), the curve disappears. Conditions that lead to postural scoliosis : • Short leg • Pelvic tilt due to contracture of the hip • Local muscle spasm @ prolapsed lumbar disc
Classification Structural Scoliosis It is always accompanied by bony abnormality or vertebral rotation. The deformity is fixed and does not disappear with change in posture. Secondary curves nearly always develop to counterbalance the primary later, they may become fixed too.
Types of Structural Scoliosis • Scoliosis due to known causes 20% • Osteopathic: due to Congenital vertebral anomalies. Rare but dangerously progressive • Neuropathic: due to asymmetrical muscle weakness (e.g. in cerebral palsy and Poliomyelitis) • 3. Myopathic: seen in the rare muscular dystrophies • 4. Neurofibromatosis: associated with severe deformity • Idiopathic scoliosis 80% • Infantile <3yrs • Juvenile 4-9 yrs • Adolescent >10yrs (Most common)
Patterns of Idiopathic Scoliosis • Infantile thoracic: • 60% male • 90% convex to the left • Associated with ipsilateral plagiocephaly (Oblique lateral deformity of the skull ) • May be resolving or progressive(severe) • Adolescent thoracic: • 90% female • 90% convex to the right • Rib rotation exaggerates the deformity • 50% develop curves of greater than 70˚
Thoracolumbar: • Slightly more common in females • Slightly more common to right • Features mid-way between adolescent thoracic and lumbar • Lumbar: • More common in females • 80% convex to left • One hip prominent but no ribs to accentuate the deformity. Therefore not noticed early, but backache in adult life E. Combined: Two primary curves, one in each direction. Even when radiologically severe, clinical deformity relatively slight because always well balanced.
Clinical features The symptoms of scoliosis can include: • Pain is common in adulthood, especially if left untreated • One of the major complaints from parents and patients is cosmetic deformity. • Uneven musculature on one side of the spine • A rib "hump" and/or a prominent shoulder blade, caused by rotation of the ribcage in thoracic scoliosis • Uneven hip and shoulder levels • Asymmetric size or location of breast in females • Unequal distance between arms and body • Clothes that do not "hang right", i.e.. with uneven hemlines • Slow nerve action (in some cases)
Physical Examination • Patients who initially present with scoliosis are examined to determine if there is an underlying cause of the deformity. During a physical examination, the following is assessed: • Skin for café au lait spots indicative of neurofibromatosis • The feet for cavovarusdeformity • Abdominal reflexes • Muscle tone for spasticity • The patient's gait is assessed • The back for signs of spina bifida • The patient is asked to bend forward (Adam's Bend Test). If a hump is noted, then scoliosis is a possibility and the patient should be sent for an x-ray to confirm the diagnosis.
Investigations Many radiologists and doctors when suspecting scoliosis will exclaim "scolie and AP-Lateral", which are two types of X-ray. • A scolie is an X-ray taken from the rear. • An AP-Lateral is taken from the side.
Cobb’s Angle Measurement used for evaluation of curves in scoliosis on an AP radiographic projection of the spine. When assessing a curve, the apical vertebra is first identified, the end or transitional vertebra are then identified through the curve above and below. • The apical vertebra is most likely displaced and rotated vertebra with the least tilted end plate. • The end/transitional vertebra is most superior and inferior vertebra which are least displaced and rotated and have the maximally tilted end plate. A line is drawn along the superior end plate of the superior end vertebra and a second line drawn along the inferior end plate of the inferior end vertebra.
Treatment • The aim: • prevent the curve becoming severe • correcting the existing deformities • A period of preliminary observation may be needed before deciding between conservative and operative treatment. • At 4-monthly intervals the patient is examined, photographed and X-rayed so that the curves can be measured and checked for progression. • School screening should permit early diagnosis and regular assessment of the need for active treatment.
Conservative treatment • If the patient is approaching skeletal maturity and the deformity <30 degree , treatment is unnecessary (Only exercises). • If the curve b/w 20 – 30 degree and in progression a support as Milwaukee brace is needed: • Thoracic support consisting of pelvic corset connected by adjustable steel supports to a cervical ring carrying occipital and chin pads • Its purpose is to reduce the lumbar lordosis and encourage active stretching and straightening of thoracic spine .
Surgical Treatment • The aim of surgery is to: • Reduce deformity • Maintain reduction by arthrodesis (The surgical immobilization of a joint (joint fusion). • Indications: • Curves >30 degree with progression • Milder curves that deteriorate significantly despite conservative treatment
KYPHOSIS Definition The term kyphosis is used to describe both; • The normal (the gentle rounding of the dorsal spine) and • The abnormal (excessive dorsal curvature). In the latter sense it signifies a well-recognized deformity which may be progressive
Classification Postural kyphosis It is common (‘round back’ or ‘drooping shoulders’) and may be associated with other postural defects such as flat-feet Structural kyphosis Is fixed and associated with changes in the shape of the vertebrae. It may occur in osteoporosis of the spine (the commonly round back of elderly people), in ankylosing spondylitis and in scheuermann’s disease (adolescent kyphosis)
Kyphos (or Gibbus) Is a Sharp posterior angulation due to localized collapse or wedging of one or more vertebrae. This may be a result of congenital defect, a fracture, or spinal tuberculosis Medical ppt http://hastaneciyiz.blogspot.com