Download
1 / 82
890 likes | 2.34k Views
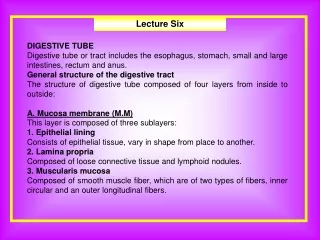
Nasogastic tube. Out line . Define the nasogastric tube Discuss the types of nasogastric tube . List the purpose of using the nasogastric tube Discuss insertion nasogastric tube Discuss removing nasogastric tube Discuss administering a tube feeding Discuss Irrigating Nasogastric Tube

E N D
Out line • Define the nasogastric tube • Discuss the types of nasogastric tube . • List the purpose of using the nasogastric tube • Discuss insertion nasogastric tube • Discuss removing nasogastric tube • Discuss administering a tube feeding • Discuss Irrigating Nasogastric Tube • Explain the procedure. • List the potential complications of Nasogastric Tube. • Demonstrate the procedure.
Introduction • Gastrointestinal intubation is inserting of rubber or plastic tube into the stomach , duodenum or intestinal • The tube inserted through mouth .nose , or abdominal ( gastrostomy .jejunostomy ) • The tube short , medium , long
Types of Tubes • Short- Nasogastric tube • Introduced from the nose to the stomach • Levin and Gastric (Salem) Sump • Used to remove gas and fluid from the upper GI tract or to obtain a specimen of gastric contents • Sometimes used for medications or feedings ( gavage )
Levin Tube • Single Lumen (hollow part of tube) • Size 14-18 French • Made of plastic or rubber with opening near tip • It is 125 cm long • Circular markings on the tube serve as insertion guides
Gastric (Salem) Sump • Gastric sump tube ( salem. Ventrole) • Double lumen catheter .clear plastic • Plastic, 12-18 FR. • It is 120 cm long • Used to decompress the stomach, keeps it empty
Smaller, inner tube (blue pigtail) vents the larger suction-drainage tube to the atmosphere by way of an opening at the distal end of the tube. Keeps the suction force at the drainage openings at less that 25 mm Hg to prevent capillary irritation. Connected to low continuous suction. Vent lumen kept above the client’s waist.
Medium tubes. • Medium length- nasoenteric used for feeding. Example- Dobhoff • Placed in the duodenum or jejunum by fluoroscopy (x-ray dept) or at client’s bedside. • Verified by x-ray before feedings begin. May take up to 24 hrs. • to pass through the stomach into the intestines. • Place client on right side to facilitate passage
Long- nasoenteric tubes. • Long- nasoenteric tubes introduced through the nose and passed through the esophagus and stomach into the intestinal tract. • Used to aspirate intestinal contents-ie. gas and fluid • Used to (Decompression) to prevent intestinal obstruction. • Due to peristalsis, prevents vomiting, reduces tension at the incision line and prevents obstruction.
Long- nasoenteric tubes. • Examples of long tubes: • Miller- Abbott- • is double lumen ( 12--- 18 fr ) 300 cm rubber tube • one lumen used for aspiration and other for Introduce with mercury, water, or saline
Long- nasoenteric tubes • Harris- • Is single lumen ( 14 fr ) • used for suction and irrigation • mercury-weighted of about 180 cm • This tube metal tip that lubricate • This use for irrigation & suction .
Long- nasoenteric tubes • Cantor tube – • has a large balloon at distal end of tube. Filled with • 4- 5 ml of mercury, water or saline to weight the tube • It is 300 cm long
Definition • Tube inserted through the nose into stomach
Purposes: • To administer tube feedings and medications to clients unable to eat by mouth or swallow a sufficient diet without aspirating food or fluids into the lungs • To establish a means for suctioning stomach contents to prevent gastric distention ,nausea, and vomiting. • To remove stomach contents for laboratory analysis • To lavage(wash)the stomach in case of poisoning or overdose of medications.
Purposes • To drain fluid or air from the stomach. • To promote healing after bowel surgery. • To monitor bleeding in the gastrointestinal (GI) tract. • To help treat an intestinal obstruction.
Assessment & Preparations: • Assessment & Prepare the client • Presence of gag reflex • Mental status or ability to cooperate with procedure • Check physician's order for insertion of NG tube. • Explain procedure to patient. • Assist the patient to high Fowler's position. • Drape chest with disposable pad
Assess the client nares • Ask client to hyperextend the head & using flashlight • Observe ( intactness of tissue nostrils including any irritation or abrasion ) • Examine the patient’s nostril for septal deviation. To determine which nostril is more patent, ask the patient to occlude each nostril and breathe through the other • Patency of nares & intactness of nasal tissue ( note especially history of nasal surgery or deviated septum )
Assess & prepare the tube • If rubber tube : • used placed it on ice for 5 to 10 minutes • This stiffens the tube , facilitating insertion • If plastic tube • Used place it in warm water until tube softer & more flexibility , facilitating insertion
Equipments: • Nasogastric tube • Adult - 16-18F • Viscous lidocaine 2% • Oral analgesic spray (Benzocaine spray or other) • Oral syringe, 12 mL • Glass of water with a straw • Water-based lubricant
Equipments: • Non allergenic adhesive Tape 2,5 cm wide • Emesis basin or plastic bag • Wall suction, set to low intermittent suction • Suction tubing and container • Flashlight . • Stethoscope. • Toomey syringe (20 to 50 ml) . • Tissues • Disposable pad & gloves . . • Tongue blade . • Normal saline solution (for irrigation only).
Note • A nasogastric (NG) tube is used for the procedure. The placement of an NG tube can be uncomfortable for the patient if the patient is not adequately prepared with anesthesia to the nasal passages and specific instructions on how to cooperate with the operator during the procedure
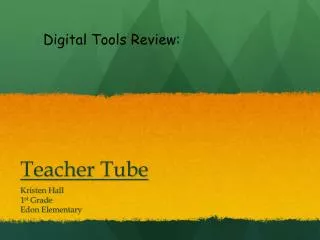
Determine how far to insert the tube • Measure the distance to insert tube by placing tip of tube at client's nostril and extending to tip of ear lobe and then to tip of xiphoid process. • Mark tube with piece of tape.
Estimation of nasogastric tube length from nostril to stomach
Insert the tube • Prepare equipment. • Wash hands. • Wear disposable gloves. • Instill 10 mL of viscous lidocaine 2% (for oral use) down the more patent nostril with the head tilted backwards, and ask the patient to sniff and swallow to anesthetize • Lubricate tip of tube with water soluble lubricant. • Ask client to lift head, and insert tube into nostril while directing tube upward and backward.
Cont,, • If client gag when tube reaches pharynx, provide tissues for tearing or watering of eyes. • When pharynx is reached, instruct client to touch chin to chest. • Encourage client to sip water through a straw or swallow even if no fluids are permitted.
Patient flexing his neck and drinking water while a nasogastric tube is inserted.
Advance tube in downward and backward direction when client swallows. Stop when client breathes. If gagging and coughing persist, check placement of tube with tongue blade and flash light. Keep advancing tube until tape marking is reached. Do not use force, rotate tube if it meets resistance. Discontinue procedure and remove tube if there are signs of distress, such as gasping, coughing, cyanosis, and inability to speak or hum.
Confirming Placement • Tube placement is confirmed prior to any use of the tube for suction, irrigation, medication admin. or feedings. • Initially, an x-ray should be ordered to confirm placement of weighted feeding tubes (Dobhoff). • Verify NG or Salem Sump tubes by auscultation of an injected air bolus over the epigastrium or aspirate stomach contents. • Measurement of tube length, visual inspection and measuring of the aspirate pH is also recommended.
Securing the GI tube • Use a skin barrier to prep the skin • Use NG strip or place a piece of tape under the tube at the nose and secure to the skin, place another piece of tape over the first piece. • Secure tube to client’s gown with a safety pin.
Document • Document: Tube type and size • Drainage or aspirate (residuals) amount, color and consistency • Irrigation type and amount • Suction- type and level (i.e. low intermittent) • Feeding- type and amount • Patient tolerance • Patient/ Family education and response
NG Suction • Tube for decompression will be attached to Intermittent Suction- keep suction between 20-80mm Hg. • Continuous suction greater than 25mm Hg can cause damage to the gastric mucosa. • Do not clamp or plug the vent lumen. • A soft hissing sound will be heard from the vent lumen if it’s patent. • Record amt. on I&O.
Conte,,, • Remove disposable gloves. • Wash hands. • Remove all equipment. • Keep the client at comfortable position. • Assist with or provide oral hygiene at regular intervals.
Complications • The main complications of NG tube insertion :- • aspiration and tissue trauma. • Placement of the catheter can induce gagging or vomiting, Patient discomfort • Epistaxis • Pulmonary complication • Esophageal perforation
Contraindications • Absolute contraindications • Severe mid face trauma • Recent nasal surgery • Relative contraindications • Coagulation abnormality • Esophageal varicose or stricture • Alkaline ingestion
Procedure of Administering a Tube Feeding.
Tube Feedings • Meet nutritional needs when oral intake not possible • Advantageous over TPN • GI integrity is preserved • Normal insulin/glucagon ratios are maintained • Admin. intermittent, continuous • Accessed by nasogastric, nasoenteric, gastrostomy or jejunostomy tube
Assessment • Before a nasogastric or orogastric feeding determine type amount frequency of feeding & tolerance of previous feeding • Assessment signs of malnutrion or dehydration • Assess allergies to any food • Presence bowel sound • Any tolerance of previous feeding ( delayed gastric empty , abdominal distention . Constipation )
Purposes: • To restore or maintain nutritional status. • To administer medications.
Equipments: • Feeding container. • Large syringe with plunger or calibrated plastic feeding bag with tubing or Prefilled bottle with a drip chamber tubing & flow regulator clamp • Stethoscope. Disposable gloves. Alcohol swab. • Toomey syringe 20 to 50 ml with adaptor . • Water for irrigation or normal saline. • Emesis basin • Feeding pump as required