Download

1 / 28
290 likes | 438 Views
Immunization. Milestones in immunization. 3000BC Evidence of sniffing powdered small pox crust in Egypt. 1500BC Turks introduce variolation. 1700AD Introduction of variolation in England and later in the US. 2000BC Sniffing of small pox crust in China. Introduction of variolation.

E N D
Milestones in immunization • 3000BC • Evidence of sniffing powdered small pox crust in Egypt • 1500BC • Turks introduce variolation • 1700AD • Introduction of variolation in England and later in the US • 2000BC • Sniffing of small pox crust in China
Introduction of variolation The wife of the British Ambassador in Turkey, in March 1717 wrote, following the variolation of her son, to a friend in England: “The small pox, so fatal, so general amongst us, is entirely harmless here by the invention of ingrafting….I am patriot enough to bring this invention into fashion in England.
Milestones in immunization • 1780AD • Edward Jenner discovers small pox vaccine
Edward Jenner Discovery of small pox vaccine
Modern era of the vaccine • 1885 • Rabies vaccine (Pasteur) • 1934 • Pertussis • 1955 • Salk polio • 1920s • Diphtheria and Tetanus
Modern era of the vaccine • 1960s • Mumps measles and rubella virus • Sabin polio • 1985 • Haemophilus • 1990s • Hepatitis and varicella • 2000 • Human Papillomavirus • (HPV)
Pre- & post-vaccine incidence of common preventable diseases
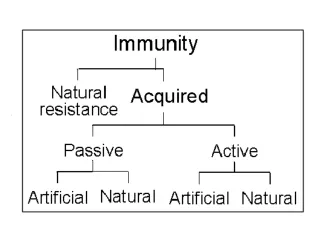
Acquired Natural resistance Passive Active Artificial Artificial Natural Natural Different modes of acquiring immunity Immunity
Natural Artificial Passive Immunity Placental transfer of IgG Antibodies or immunoglobulins Colostral transfer of IgA Immune cells
disease diphtheria, tetanus human, horse antibody source indication human vericella zoster horse gas gangrene, botulism, snake bite, scorpion sting prophylaxis, therapy immunodeficiencies post-exposure post-exposure human human rabies, prophylaxis hypogamma-globulinemia Passive Immunization
Disadvantages Advantages Advantages and Disadvantages of Passive Immunization no long term protection serum sickness immediate protection risk of hepatitis and Aids graft vs. host disease (cell graft only)
Artificial Natural Active Immunization Attenuated organisms killed organisms exposure to sub-clinical infections sub-cellular fragments toxins others
Live Attenuated Vaccines • polio* • not used in std. schedule • hepatitis A • standard 2006 measles, mumps & rubella • yellow fever • Military and travelers • Varicella zoster • children with no history of chicken pox • Influenza • selected age group (5-49) • tuberculosis • not used in this country
Killed Whole-Organism Vaccines polio • Q fever • population at risk • influenza • elderly and at risk • typhoid, cholera, plague • epidemics and travelers • pertussis • replaced by the acellular vaccine • rabies • post exposure
Microbial Fragment Vaccines • Bordetella. Pertussis • virulence factor protein • Haemophilus influenzae B • protein conjugated polysaccharide • Streptococcus pneumoniae • Polysaccharide mixture • Neisseria meningitidis • polysaccharide
Microbial Fragment Vaccines • Clostridium tetani (tetanus) • inactivated toxin (toxoid) • Corynebacterium diphtheriae • inactivated toxin (toxoid) • Vibrio cholerae • toxin subunits • Hepatitis B virus • cloned in yeast
chemical modification toxin moiety antigenic determinants Modification of Toxin to Toxoid Toxin Toxoid
Future Vaccines • anti-Idiotype Vaccine DNA Immuno-dominant peptide
Antiidiotype antibody in tolerance Antiidiotype antibody production Antiidiotype mediated tolerance
Adjuvants Adjuvant type Human use Mode of action • Salts: • Al(OH)3; AlPO4; CaPO4 • Be(OH)2 • Yes • Yes • No Slow release of antigen; TLR interaction and cytokine induction • Mineral oils without bacteria • No Slow release of antigen • Bacteria in Mineral oils (Mycobacteria, Nocardia) Slow release of antigen TLR interaction and cytokine induction • Yes • No
Adjuvants Adjuvant type Human use Mode of action • Bacteria: • Bordetella pertussis • Mycobacterium bovis • (BCG and others) • Yes TLR interaction and cytokine induction • No • Bacterial products: • Myramyl peptides TLR interaction and cytokine induction • No • Synthetic polymers: • Liposomes • ISCOM • Poly-lactate • No Slow release of antigen
Adjuvants Adjuvant type Human use Mode of action • Poly-nucleotides: • CpG TLR interaction and cytokine induction • No* • Cytokines: • IL-1, IL-2, IL-12, IFN-γ, etc. Activation of T and B cells and APC • No* • *Used in experimental immunotherapy of human malignancies
Recommended Childhood Immunization Schedule Recommended age range Catch-up immunization Certainigh risk groups MMWR, 55: Jan 5, 2007
Recommended Immunization Schedule for Ages 7-18 Recommended age range Catch-up immunization Certainigh risk groups MMWR, 55: Jan 5, 2007
Event Frequency • local • redness, swelling, pain 1 in 2-3 doses • systemic: Mild/moderate • fever, drowsiness, fretfulness vomiting • anorexia 1 in 2-3 doses 1 in 5-15 doses • systemic: more serious • persistent crying, fever • collapse, convulsions • acute encephalopathy • permanent neurological deficit 1 in 100-300 doses 1 in 1750 doses 1 in 100,000 doses 1 in 300,000 doses Adverse Events OccurringWithin 48 Hours DTP of Vaccination