Download
1 / 1
10 likes | 138 Views
Abstract WEPE0151 :. improvement. improvement. improvement. no change. no change. no change. worsening. worsening. worsening.

E N D
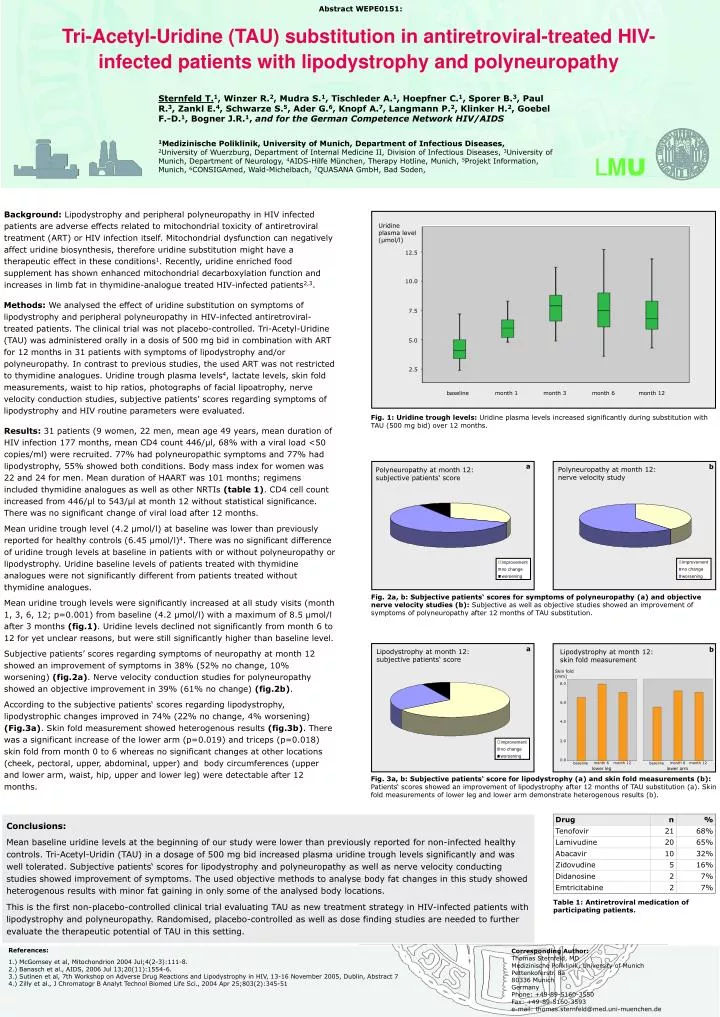
Abstract WEPE0151: improvement improvement improvement no change no change no change worsening worsening worsening Sternfeld T.1, Winzer R.2, Mudra S.1, Tischleder A.1, Hoepfner C.1, Sporer B.3, Paul R.3, Zankl E.4, Schwarze S.5, Ader G.6, Knopf A.7, Langmann P.2, Klinker H.2, Goebel F.-D.1, Bogner J.R.1, and for the German Competence Network HIV/AIDS 1Medizinische Poliklinik, University of Munich, Department of Infectious Diseases, 2University of Wuerzburg, Department of Internal Medicine II, Division of Infectious Diseases, 3University of Munich, Department of Neurology, 4AIDS-Hilfe München, Therapy Hotline, Munich, 5Projekt Information, Munich, 6CONSIGAmed, Wald-Michelbach, 7QUASANA GmbH, Bad Soden, Tri-Acetyl-Uridine (TAU) substitution in antiretroviral-treated HIV-infected patients with lipodystrophy and polyneuropathy LMU Background: Lipodystrophy and peripheral polyneuropathy in HIV infected patients are adverse effects related to mitochondrial toxicity of antiretroviral treatment (ART) or HIV infection itself. Mitochondrial dysfunction can negatively affect uridine biosynthesis, therefore uridine substitution might have a therapeutic effect in these conditions1. Recently, uridine enriched food supplement has shown enhanced mitochondrial decarboxylation function and increases in limb fat in thymidine-analogue treated HIV-infected patients2,3. Uridine plasma level (µmol/l) 12.5 10.0 Methods: We analysed the effect of uridine substitution on symptoms of lipodystrophy and peripheral polyneuropathy in HIV-infected antiretroviral-treated patients. The clinical trial was not placebo-controlled. Tri-Acetyl-Uridine (TAU) was administered orally in a dosis of 500 mg bid in combination with ART for 12 months in 31 patients with symptoms of lipodystrophy and/or polyneuropathy. In contrast to previous studies, the used ART was not restricted to thymidine analogues. Uridine trough plasma levels4, lactate levels, skin fold measurements, waist to hip ratios, photographs of facial lipoatrophy, nerve velocity conduction studies, subjective patients’ scores regarding symptoms of lipodystrophy and HIV routine parameters were evaluated. 7.5 5.0 2.5 baseline month 1 month 3 month 6 month 12 Fig. 1: Uridine trough levels: Uridine plasma levels increased significantly during substitution with TAU (500 mg bid) over 12 months. Results: 31 patients (9 women, 22 men, mean age 49 years, mean duration of HIV infection 177 months, mean CD4 count 446/µl, 68% with a viral load <50 copies/ml) were recruited. 77% had polyneuropathic symptoms and 77% had lipodystrophy, 55% showed both conditions. Body mass index for women was 22 and 24 for men. Mean duration of HAART was 101 months; regimens included thymidine analogues as well as other NRTIs (table 1). CD4 cell count increased from 446/µl to 543/µl at month 12 without statistical significance. There was no significant change of viral load after 12 months. Mean uridine trough level (4.2 µmol/l) at baseline was lower than previously reported for healthy controls (6.45 µmol/l)4. There was no significant difference of uridine trough levels at baseline in patients with or without polyneuropathy or lipodystrophy. Uridine baseline levels of patients treated with thymidine analogues were not significantly different from patients treated without thymidine analogues. Mean uridine trough levels were significantly increased at all study visits (month 1, 3, 6, 12; p=0.001) from baseline (4.2 µmol/l) with a maximum of 8.5 µmol/l after 3 months (fig.1). Uridine levels declined not significantly from month 6 to 12 for yet unclear reasons, but were still significantly higher than baseline level. Subjective patients’ scores regarding symptoms of neuropathy at month 12 showed an improvement of symptoms in 38% (52% no change, 10% worsening) (fig.2a). Nerve velocity conduction studies for polyneuropathy showed an objective improvement in 39% (61% no change) (fig.2b). According to the subjective patients‘ scores regarding lipodystrophy, lipodystrophic changes improved in 74% (22% no change, 4% worsening) (Fig.3a). Skin fold measurement showed heterogenous results (fig.3b). There was a significant increase of the lower arm (p=0.019) and triceps (p=0.018) skin fold from month 0 to 6 whereas no significant changes at other locations (cheek, pectoral, upper, abdominal, upper) and body circumferences (upper and lower arm, waist, hip, upper and lower leg) were detectable after 12 months. a b Polyneuropathy at month 12: nerve velocity study Polyneuropathy at month 12: subjective patients‘ score Fig. 2a, b: Subjective patients‘ scores for symptoms of polyneuropathy (a) and objective nerve velocity studies (b): Subjective as well as objective studies showed an improvement of symptoms of polyneuropathy after 12 months of TAU substitution. a b Lipodystrophy at month 12: subjective patients‘ score Lipodystrophy at month 12:skin fold measurement Skin fold (mm) 8.0 6.0 4.0 2.0 0.0 month 6 month 12 month 6 month 12 baseline baseline lower leg lower arm Fig. 3a, b: Subjective patients‘ score for lipodystrophy (a) and skin fold measurements (b): Patients‘ scores showed an improvement of lipodystrophy after 12 months of TAU substitution (a). Skin fold measurements of lower leg and lower arm demonstrate heterogenous results (b). Conclusions: Mean baseline uridine levels at the beginning of our study were lower than previously reported for non-infected healthy controls. Tri-Acetyl-Uridin (TAU) in a dosage of 500 mg bid increased plasma uridine trough levels significantly and was well tolerated. Subjective patients‘ scores for lipodystrophy and polyneuropathy as well as nerve velocity conducting studies showed improvement of symptoms. The used objective methods to analyse body fat changes in this study showed heterogenous results with minor fat gaining in only some of the analysed body locations. This is the first non-placebo-controlled clinical trial evaluating TAU as new treatment strategy in HIV-infected patients with lipodystrophy and polyneuropathy. Randomised, placebo-controlled as well as dose finding studies are needed to further evaluate the therapeutic potential of TAU in this setting. Table 1: Antiretroviral medication of participating patients. References: 1.) McGomsey et al, Mitochondrion 2004 Jul;4(2-3):111-8. 2.) Banasch et al., AIDS, 2006 Jul 13;20(11):1554-6. 3.)Sutinen et al, 7th Workshop on Adverse Drug Reactions and Lipodystrophy in HIV, 13-16 November 2005, Dublin, Abstract 7 4.) Zilly et al., J Chromatogr B Analyt Technol Biomed Life Sci., 2004 Apr 25;803(2):345-51 Corresponding Author: Thomas Sternfeld, MD Medizinische Poliklinik, University of Munich Pettenkoferstr. 8a 80336 Munich Germany Phone: +49-89-5160-3550 Fax: +49-89-5160-3593 e-mail: thomas.sternfeld@med.uni-muenchen.de