Download
1 / 28
450 likes | 1.5k Views
Helicobacter pylori Infection: Who to test and When to Treat. Ahmed Laving Paediatric Gastroenterologist and Senior Lecturer University of Nairobi. Outline. Epidemiology Risk Factors Pathology Clinical Outcomes Diagnosis Management Conclusion. Epidemiology: H pylori.

E N D
Helicobacter pylori Infection: Who to test and When to Treat Ahmed Laving Paediatric Gastroenterologist and Senior Lecturer University of Nairobi
Outline • Epidemiology • Risk Factors • Pathology • Clinical Outcomes • Diagnosis • Management • Conclusion
Epidemiology: H pylori • The most widespread chronic infection in manwith a worldwide distribution • Estimated that half of the human population is infected • >50% of children infected by 10 years of age and prevalence rises to >80% in young adults in developing countries • Locally: prevalence of 45% in children under 3 years of age and 80% in children 3-15 years of age • Ford AC, Epidemiology of Hpylori infection and Public Health Implications. Helicobacter. 2010; 15;Nabwera HM, Prevalence of H pylori infection in Kenyan schoolchildren aged 3-15 years. Eur J Gastroenterology Hepatol. 2000;12(5).Langat AC. Prevalence of H pylori in children less than three years of age in health facilities in Nairobi Province. East Afr Med J. 2006;83(9)
Risk Factors and Transmission • Socioeconomic status and living conditions in early life • Overcrowding • Number of siblings • Sharing a bed • Lack of running water • Transmission: • Unknown! • Person to person (fecal/oral or oral/oral exposure) • Intra-familial clustering
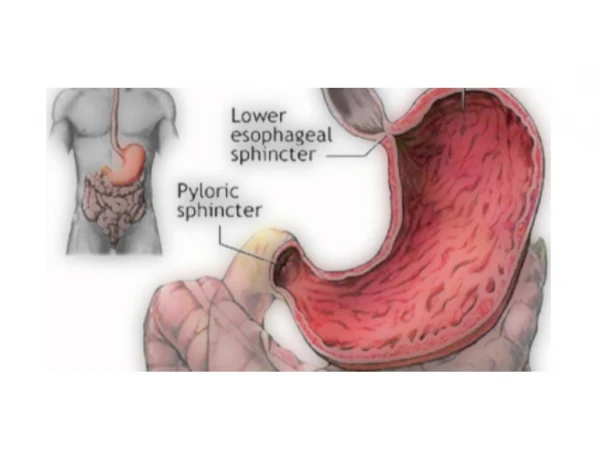
Pathology 1.H. pylori penetrates the mucus layer of hosts stomach and adheres to the surface of gastric mucosal epithelial cells. It then produces ammonia from urea; 2. The ammonia protects the bacterium by neutralizing gastric acid; 3. Proliferation, migration, and formation of infectious focus; 4. Gastric ulcer results from destruction of mucosa, inflammation and mucosal cell death.
Children are not small adults! Prevalence rates different Fewer complications including peptic ulcers Gastric malignancies very rare Higher rates of antibiotic resistance Differential diagnosis for abdominal pain is different Debate over whether H pylori gastritis causes pain in the absence of PUD ?Protective immunological role of H pylori infection
1. Who should be tested? 2. What tests? 3. Who should be treated? 4. What treatment regimens?
Who to test? • Child with acute GE? • Child with recurring peri-umbilical pain? • Child with acute onset vomiting after eating out at a roadside hotel? • Child with supra-pubic pain?
1. Who should be tested? • Abdominal pain SITE: Epigastric: YES Periumbilical/lower abdomen: NO DURATION: Acute onset? NO! Chronic? YES, if epigastric • Diarrhoeal illness? NO • Family history • PUD • Gastric carcinoma • Non GI conditions? • Iron deficiency anaemia • Otitis media • Dental disease • Idiopathic thrombocytopenic purpura
H pylori and Abdominal Pain • Functional abdominal pain very common amongst children • Related to social and familial factors • Meta analysis of 45 studies in children with recurring abdominal pain • NO association with H pylori infection! • Study on children with dyspepsia undergoing OGD • Majority had reflux and improved with antacid therapy • H pylori eradication not associated with symptom improvement • H pylori status NOT associated with abdominal pain Levine A. Pediatrics 2004;113 Macarthur C. Helicobacter pylori infection and childhood recurrent abdominal pain: lack of evidence for a cause and effect relationship. Can J Gastroenterol 1999;13: ode G, Brenner H, Adler G, et al. Recurrent abdominal pain in children: evidence from a population-based study that social and familial factors play a major role but not Helicobacter pylori infection. J Psychosom Res 2003;54:417–21
Who to test? Guideline Recommendations • DYSPEPTIC signs and symptoms for >8 weeks* • Primary goal to determine underlying cause of abdominal pain, NOT simply the presence of H pylori infection • Diagnostic testing for H pylori infection NOT recommended in children with functional abdominal pain, acute GE* • Testing for H pylori may be considered in: • Children with refractory iron deficiency anaemia • Children with first degree relatives with gastric cancer • insufficient evidence that H pylori infection is causally related to otitis media, periodontal disease, idiopathic thrombocytopenic purpura
2. What tests? • Invasive • OGD with biopsies for histopathology, rapid urease tests, culture • Non invasive • Serology • Urea breath test • Stool H pylori antigen
Diagnosis • Invasive testing: • OGD/Histology: Gold standard, Strong Recommendation • However, ?feasible to scope every child with dyspepsia in developing countries
Diagnosis • Non invasive testing: • Ideally should be restricted to epidemiologic studies • For checking response to treatment 4 to 8 weeks after completion • Avoided as pre-diagnostic method in patients with typical signs and symptoms
Non invasive tests 1. Monoclonal Stool antigen Test - High sensitivity (98%) and specificity (99%) • Excellent tool in confirming eradication of H pylori 2. Urea Breath Test (UBT) • High sensitivity (96%) and specificity (93-97%) in patient > 6 yrs • Most useful application is to verify eradication of the infection 3. Serology Tests (ELISA IgG) • Poor sensitivity - Antibody levels persist for many months
What tests? Guideline Recommendations • Initial diagnosis of H pylori infection ideallybased on positive histopathology, rapid urease test or a positive culture • A validated ELISA H pylori antigen in stool is a reliable noninvasive test to determine whether H pylori has been eradicated • 13C-Urea Breath Test is a reliable noninvasive test to determine whether H pylori has been eradicated • Serology tests (IgG, IgA) against H pylori in serum, whole blood, urine, and saliva not reliable for use in clinical setting for paediatric patients
3. Who to treat? Guideline Recommendations • A ‘test and treat’ strategy is NOT recommended in children, unlike adult guidelines • Treatment recommended in children with H pylori positive peptic ulcer disease • Treatment may be considered in children with H pylori detected by biopsy-based methods • Treatment ideally based on sensitivity patterns • H pylori detected by stool antigen or serology? To treat or not to treat???
4. What Treatment Regimens? First Line: Triple therapy Dosages Amoxicillin: 50 mg/kg/day Clarithromycin: 20 mg/kg/day Metronidazole: 20 mg/kg/day Bismuth salt: 8 mg/kg/day Omeprazole: 1-2 mg/kg/day • PPI + Amoxicillin + Clarithromycin • PPI + Amoxicillin + Metronidazole • PPI + Amoxicillin + Bismuth Duration of treatment: 14 days
Treatment Failure and Rescue Treatment Plan Reasons for Treatment Failure • Host genetic factors • H pylori virulent factors • Antibiotic resistance • Inadequate compliance • Insufficient duration of Rx • Household crowding? Rescue Treatment Strategies • Check antibiotic resistance status • Longer Rx duration • Avoid previously used antibiotics • Use sequential or quadruple Rx • Ensure patient compliance • Screen family members
Assessment of eradication • 10 year old with peri-umbilical pain; treated for H. pylori. Returns after 2 weeks with no change in abdominal pain. What next? • Repeat stool H. pylori Ag test; if positive, retreat with “ESOKIT” • Continue PPI • Refer!
Eradication • Aim: to achieve >90% eradication with first line Rx • Re-infection rates with appropriate treatment usually less than 1-2% • Eradication assessed with stool antigen or breath tests • When: • 2 weeks after completing PPI • 4-6 weeks after completing antibiotics • 8 WEEKS AFTER COMPLETING TREATMENT! • If abdominal pain persists, H pylori was probably NOT the cause in the first place
Second Line Therapy • Recommended 2nd line therapy: Quadruple regimen of amoxicillin, metronidazole/clarithromycin, a bismuth salt and a PPI • Quadruple regimens more effective as 2nd line therapy when a 1st line triple regimen failed to eradicate infection • Meta‐analysis of five RCTs (576 subjects) showed superiority of quadruple over triple therapy (pooled OR = 2.86; 95% CI: 1.73‐4.73) • Other options: PPI, levofloxacin, and amoxicillin for 10 days • More effective and better tolerated than bismuth quadruple therapy • However, quinolones not recommended in children
2nd line therapy: other options • PPI, levofloxacin, and amoxicillin for 10 days • More effective and better tolerated than bismuth quadruple therapy • However, quinolones not recommended in children • Sequential therapy • PPI + Amoxiciilin for 5 days, then • PPI, Metronidazole, Clarithromycin for 5 days • As effective as 7 day course of triple therapy
3rd and 4th Line Therapies • If H pylori infection persists after a second course of treatment: • Is eradication of H pylori necessary? • Refer to a specialist for culturing H pylori and performing sensitivity testing • Quinolones (levofloxacin/moxifloxacin), amoxicillin/tetracycline, rifabutin and furazolidone • High‐dose PPI plus amoxicillin and levofloxacin or rifabutin therapy has been associated with high rates of eradication • Rifabutin only as 4th line option
Conclusions • H pylori NOT associated with functional abdominal pain • Test and treat strategy NOT recommendedin children • If suspecting PUD, endoscopy for histologic/urea test recommended for diagnosis • Triple therapy for 14 days; ensure compliance • Quadruple therapy as second line • Stool H pylori test (or urea breath test) to confirm eradication • 2 weeks after completing PPI • 4-6 weeks after completing antibiotics