Download
1 / 93
930 likes | 1.41k Views
THE OVERWHELMING CHALLENGE OF COMMUNITY ASSOCIATED METHICILLIN RESISTANT STAPHYLOCOCCUS AUREUS ( CA-MRSA ). George S. Kotchmar, Jr., M.D., FAAP Colonel, USAF, Retired Professor of Clinical Pediatrics Director, Division of Infectious Diseases – Dept. of Pediatrics

E N D
THE OVERWHELMING CHALLENGE OF COMMUNITY ASSOCIATED METHICILLIN RESISTANTSTAPHYLOCOCCUS AUREUS (CA-MRSA) George S. Kotchmar, Jr., M.D., FAAP Colonel, USAF, Retired Professor of Clinical Pediatrics Director, Division of Infectious Diseases – Dept. of Pediatrics University of South Carolina School of Medicine
OBJECTIVES • DESCRIBE THE EPIDEMIOLOGY DEFINING COMMUNITY – BASED MRSA INFECTION • UNDERSTAND LABORATORY/MICROBIOLOGY STUDIES AND MRSA RESISTANCE AND TRENDS • RECOGNIZE TYPICAL AND ATYPICAL CLINICAL FEATURES OF COMMUNITY MRSA INFECTIONS IN CHILDREN • MAKE APPROPRIATE EMPIRIC AND DEFINITIVE MANAGEMENT DECISIONS OF MINOR AND SERIOUS MRSA INFECTIONS INCLUDING AN AWARENESS OF APPROPRIATE OLD AND NEW ANTIMICROBIALS • COUNSEL/ADDRESS FAMILIES ABOUT RECURRENT MRSA INFECTIONS
“COMMUNITY AWARENESS” • NEWSWEEK ARTICLE (DECEMBER 6, 2004): TRAPPING THE SUPERBUGS – “ANTIBIOTICS ARE LOSING THEIR PUNCH AS MICROBES LEARN TO RESIST THEM. CAN WE STOP THE NEW KILLERS?” • PEOPLE ARTICLE (JUNE 27, 2005): KILLER MICROBE – “DOCTORS WARN THAT AN INFECTION ONCE FOUND MOSTLY IN HOSPITALS IS SPREADING ACROSS THE COUNTRY” • THE STATE NEWSPAPER (JUNE 15, 2005): “A DOZEN FEMALE INMATES TREATED FOR SPIDER BITES”
CLASSIFICATION OF STAPHYLOCOCCUS AUREUS TYPEmecAANTIMICROBIAL SUSCEPTIBILITYVANC. MIC GENE Ox Ery Clin FQ SXT Lin Q/D Dap METHICILLIN-SUSCEPTIBLE (MSSA) (-) S S/R S S S S S S <2 METHICILLIN-RESISTANT (MRSA) COMMUNITY-ACQUIRED (CA-MRSA) (+) R S/R S S S S S S <2 HEALTHCARE-ASSOCIATED (HA-MRSA) (+) R R R R S/R S S S <2 VANCOMYCIN-INTERMEDIATE (VISA) (+/-) R R R R S S S S 8-16 VANCOMYCIN-RESISTANT (VRSA) (+) R R R R S S S S >32
MRSA HOSPITALIZATIONS, UNITED STATES • MRSA, ICU (NNISS DATA) 2003 – 59.5% / 2004 – 64% • BURDEN S. AUREUS INFECTIONS ON HOSPITALS (AGENCY FOR HEALTHCARE RESEARCH AND QUALITY, AHRQ) 2000-2001 - AVERAGE LOS 14.3D (NO S. AUREUS INFECTION 4.5D) - AVERAGE CHARGES $48,824 ($14,141) - HOSPITAL MORTALITY 11.2% (2.3%) • DIAGNOSIS MRSA INFECTION ANNUALLY 3.95 PER 1,000 HOSPITAL DISCHARGES (NATIONAL HOSPITAL DISCHARGE SURVEY, NHDS) 1999-2000 SJ Rehn and JG Bartlett CID 2006; 42 (Supp 12): S63-64 National Nosocamial Infectious Surveillance System. Am J Infect Control 2004; 32: 470-485 Noskin GA, et al. Arch Intern Med 2005; 165: 1756-1761 MJ Kuehnert, et al. Emerg Infect Dis. 2005; 11: 868-872
CDC DEFINITIONS OF CA-MRSA & HA-MRSA • CA-MRSA - PATIENT WITH MRSA INFECTION AND NOHISTORY OF THE FOLLOWING: SURGERY, HOSPITALIZATION, OR RESIDENCE IN A LONG-TERM CARE FACILITY WITHIN THE YEAR BEFORE INFECTION; PRESENCE OF PERCUTANEOUS DEVICE OR INDWELLING CATHETER; DIALYSIS WITHIN PREVIOUS YEAR; HOSPITALIZATION >48H BEFORE MRSA CULTURE; OR PREVIOUS MRSA INFECTION OR COLONIZATION • HA-MRSA – PATIENT WITH MRSA NOT PRESENT OR INCUBATING AT THE TIME OF ADMISSION TO HOSPITAL/ HCF AND EVIDENT >48 HOURS AFTER ADMISSION • “COMMUNITY ASSOCIATED” DEFINES INFECTIONS BY THEIR OCCURRENCE IN PATIENTS LACKING SPECIFIC RISK FACTORS FOR HEALTH CARE CONTACT
EVOLUTION OF MRSA PCN-R HA-MRSACA-MRSA 4 PEDS SA DEATHS DUE TO CA-MRSA SA 1942 1944 1959 1960 1990 1997 2000s PCN METHICILLIN INCREASING REPORTS OF CA-MRSA Saravolatz, et al. Annals Internal Med 1982 Chambers. Emerging Infect Dis 2001
CA-MRSA: LACK OF RISK FACTORS • CASE REPORTS OF CA-MRSA IN CHILDREN & ADULTS W/O RISK FACTORS BEGIN TO APPEAR IN EARLY 1990’S • RETROSPECTIVE REVIEW OF RISK FACTORS IN CHILDREN WITH CA-MRSA (1988-90 COMPARED WITH 1993-95) - RISK FACTORS: HOSPITALIZATION OR ABX WITHIN 6 MONTHS, HISTORY OF INTUBATION, CHRONIC CONDITION, URINARY OR VENOUS CATHETER, ANY SURGICAL PROCEDURE, OR HOUSEHOLD CONTACT WITH AN IDENTIFIED RISK FACTOR - PREVALENCE OF CA-MRSA AMONG CHILDREN WITHOUT IDENTIFIED RISK FACTORS WAS INCREASING (p<0.001) Herold, et al. JAMA Feb 1998
CA-MRSA: LACK OF RISK FACTORS(Results of Analysis) • 26-fold increase in CA-MRSA w/o identified risk factor • Similar clinical syndromes: CA-MRSA or MSSA • Susceptible to multiple non-B-lactam antibiotics • Isolates genetically distinct from traditional MRSA (PFGE) • All contained mecA gene Herold BC, et al. JAMA Feb 1998
SUMMARY FINDINGS MRSA PROJECT, 2001-2003 • OVER 12,500 CASES MRSA • CA-MRSA % VARIED BY SITE BALTIMORE 8% MINNESOTA 12% ATLANTA 20% • CA-MRSA INCIDENCE: 18-26 PER 100,000 • 6% OF CA-MRSA WAS INVASIVE • 42% OF 2,581 INTERVIEWS SUCCESSFUL WITH 280 (11%) RECLASSIFIED WITH IMPACT HA FROM 19% TO 17% Fridkin SK, et al. NEJM 2005; 352: 1436-1444
EPIDEMIOLOGY CA-MRSA – CDC 2001-2002 • 9-20% OF ISOLATES FROM 3 SURVEY AREAS, U.S. • INCIDENCE 25.7/100,000 POP. ATLANTA; 18/100,000 POP. M.D. • 77% CA-MRSA ISOLATED – SKIN/SOFT TISSUE INFECTIONS • WOUND INFECTIONS 10% OF CA-MRSA DISEASE • 4% SINUSITIS OR UTI; 3% BACTEREMIA; 2% PNEUMONIA • WHITE & BLACK CHILDREN LESS THAN 2 YEARS OLD INCIDENCE – 16/100,000 AND 70/100,000 (ATLANTA); 18/100,000 AND 40/100,000 (BALTIMORE) SK Fridkin, et al. NEngl J Med 2005; 352: 1436-1444
INVASIVE MRSA INFECTIONS INCREASINGATLANTA & BALTIMORE, 2001-2002 AND 2004(ACTIVE BACTERIAL CORE SURVEILLANCE, EIP) ATLANTABALTIMORE 2002 19/100,000 (13%CA) 40/100,000 (7%CA) 2004 33/100,000 (17%CA) 115/100,000 (24%CA) May 2006 Emory/CDC Conference with Data Courtesy of Drs. Klevens & Morrison
% OF INVASIVE MRSA CASES CLASSIFIED AS CA BY SITE, JULY - DECEMBER 2005 (CDC ABC SURVEILLANCE) • CALIFORNIA 15 • OREGON 22 • TENNESSEE 14 • GEORGIA 14 • MARYLAND 22 • MINNESOTA 10 • COLORADO 12 • CONNECTICUT 12 • NEW YORK 7 Emory U. School of Medicine & CDC “Challenges of MRSA, Community Pathogen” Conference (May 12, 2006) Atlanta, GA
INCIDENCE OF INVASIVE MRSA BY AGETN, AUG 2004-JULY 2005 PER 100,000 POPULATION • AGE 0-4 YEARS, 21; 5-9 YEARS, 3; 10-14 YEARS, 4; 15-19 YEARS, 3; 20-24 YEARS, 7 • AGE <1 YEAR, 74; 1 YEAR, 17; 2 YEARS, 8; 3 YEARS, 4; 4 YEARS, 1; 5 YEARS, 5 • INCIDENCE IN AFRICAN-AMERICANS IN AGE 0-19 YEARS 3 TO 7 TIMES GREATER Courtesy Marion Kainer, M.D. Tennessee Dept. Health, May 12, 2006, Atlanta Conference
MRSA COMPARED TO OTHER PUBLIC HEALTH PROBLEMS (CDC ACTIVE BACTERIAL CORE SURVEILLANCE PROJECT) • INCIDENCE PER 100,000 FOR INVASIVE ORGANISMS - .31NEISSERIAMENINGITIDIS - 1.4HAEMOPHILUSINFLUENZAE - 3.3 GROUP A STREPTOCOCCUS - 7.3 GROUP B STREPTOCOCCUS - 12.8 STREPTOCOCCUS PNEUMONIA • 33.4-35MRSA ABC DATA 2004
BURDEN INVASIVE BACTERIAL DISEASEABC CASES AND US PROJECTIONS 2003-2004 NATIONAL PROJECTIONS CASESCASESDEATHS NM 215 1,425 175 HI 465 3,750 550 GAS 1,222 11,275 1,800 GBS 2,116 20,375 2,175 SP 3,529 40,400 5,450 MRSA* 7,547 89,301 17,482 CDC Preliminary Estimates
CA-MRSA DISTINGUISHED FROM HCA-MRSA • EPIDEMIOLOGY – TRADITIONAL MRSA RISK FACTORS ABSENT • GENETIC RESISTANCE DETERMINANTS – METHICILLIN R CARRIED BY MOBILE STAPHYLOCOCCAL CASSETTE CHROMOSOME mec (SCCmec) TYPE IV • ANTIMICROBIAL RESISTANCE PATTERNS - RESISTANCE IS USUALLY LIMITED TO B-LACTAM ANTIMICROBIALS - IN LARGE STUDIES, MOST ISOLATES SUSCEPTIBLE TO CLINDAMYCIN, GENTAMICIN, LINEZOLID, RIFAMPIN, TCN, TMP-SX, VANCOMYCIN • PULSE FIELD TYPING – USA 300, USA 400 • VIRULENCE FACTORS – PANTON VALENTINE LEUKOCIDIN (PVL) TOXIN • CLINICAL VIRULENCE – INCREASED IN COMPARISON TO MSSA
PULSED-FIELD GEL ELECTROPHORESIS (PFGE) • CDC STUDIES OF OVER 1200 DIFFERENT ISOLATES STAPHYLOCOCCUS – PFGE • USING 80% SIMILARITY THRESHOLD, ALMOST ALL ISOLATES FELL INTO 8 PATTERNS • LINEAGE TYPES CALLED USA 100-800
PFGE CA-MRSAHCA-MRSA USA 100 4% USA 100 96% USA 300 78% USA 200 0% USA 400 0% USA 300 4% USA 500 11% USA 800 0% USA 700 0% USA 800 7%
HA-MRSA BLOOD STREAM INFECTIONS (BSIs)EMERGENCE USA300 GENOTYPEGMH 2004 • MRSA USA300 ACCOUNTED FOR 28% OF HA BSIs & 20% OF NOSOCOMIAL BSIs • RISK FACTORS FOR USA300 BSI - CONCURRENT SKIN AND SOFT TISSUE INFECTION (OR 3.67; 95% CL, 1.10-12.28) - INJECTION DRUG USE (OR 4.26; 95% CL, 1.08-16.84) Seybold, et al. CID March 2006
INVASIVE MRSA ISOLATESHA RISK FACTORS VS PFGE TYPE(ABC’S SURVEILLANCE 2004-2005) PFGE TYPENO HARF’SHARF’S>48HRS<48HRS USA300,400,1000 70% (19) 28% (8) 18% (8) USA100,200,500 26% (7) 72% (21) 80% (35) NOT TYPEABLE 4% (1) 0 2% (1) Klevens et al. SHEA 2006
MOLECULAR CHARACTERISTICS CA-MRSA DISEASE • COMPARISON CA-MRSA & HA-MRSA STRAINS REVEALED 7 EXOTOXIN GENES MORE LIKELY FOUND IN CA-MRSA STRAINS: lukS-PV, lukF-PV, sea, seb, sec, seh, sek • MORE THAN 90% OF CA-MRSA DISEASE-CAUSING STRAINS BEAR GENES ENCODING PVL • PANTON-VALENTINE LEUKOCIDIN TOXIN: PORE-FORMING CYTOLYTIC TOXIN WITH SPECIFICITY FOR LEUKOCYTES (LYSIS OF PMN CAN INITIATE RELEASE OF INFLAMMATORY MEDIATORS) • PVL ENCODED BY lukS-PV AND lukF-PV GENES THAT CAN BE TRANSFERRED BETWEEN STRAINS BY BACTERIOPHAGE • PVL PRESENT < 5% UNSELECTED S. AUREUS STRAINS; PRESENT MOST MSSA FURUNCULOSIS/MSSA NECROTIZING PNEUMONIA/NEARLY ALL CA-MRSA ISOLATES • FEW HA-MRSA STRAINS PRODUCE PVL Naimi TS, et al. J AMA, 2003; 290: 2976-2984 SE Crawford and Robert Daum. Pediatr Infect Dis J 2005; 24: 459-460
MRSA TOXIN ANALYSIS • PANTON-VALENTINE LEUKOCIDIN TOXIN (PVL) - SYNERGOHYMENOTROPIN TOXIN - COMBINATION 2 PROTEINS (lukS and F) THAT ACT SYNERGISTICALLY - POTENT MEDIATOR OF INFLAMMATION AND ACTIVATOR OF LEUKOCYTES - PVL DESTROYS LEUKOCYTES – CREATES LYTIC PORES • PVL ASSOCIATED WITH NECROTIC INFECTIONS - SKIN / SC FAT - PNEUMONIA – MORTALITY RATE 32% WITH PVL POSITIVE STRAINS / 6% WITH PVL NEGATIVE STRAINS Gillet, et al. Lancet 2002; 359: 753-759
MRSA RESISTANCE • RESISTANCE ISLANDS ARE GROUPED INTO STAPHYLOCOCCAL CHROMOSOME CASSETTE OR (SCC) mec TYPES BASED ON: • mec CLASS – A OR B • ccr – 1, 2, OR 3 • EXAMPLE – “CLASS B mec” + “TYPE 2 ccr” = “SCCmec TYPE IV” • CURRENTLY 4 SCC mec TYPES DESCRIBED IN LITERATURE * SCC mec I-IV * ~78% CA-MRSA SCCmec IV / ~78% HCA-MRSA SCCmec II
MRSA RESISTANCE SCCmec IISCCmec IV MOSTLY IN HCA-MRSA MOSTLY IN CA-MRSA CAN CARRY OTHER R GENES USUALLY DO NOT CARRY OTHER R GENES LARGE ~50KB SMALL ~20KB (LESS MOBILE/RETARDS GROWTH) (MORE MOBILE/GROWS QUICKLY) LESS COMMON IN CONS VERY COMMON IN CONS (UP TO 80%)
% SECONDARY RESISTANCE OF MRSA FROM OTHER SOURCES CA*HA*NNIS ’03 2001-03+ ERYTHROMYCIN 89.5 93.2 93.5 78.2 CIPROFLOXACIN 50 88.6 92.8 34.7 CLINDAMYCIN 29.3 65.9 76.9 14.6 GENTAMICIN 2.9 8.1 16.1 3.7 RIFAMPIN 0.5 3.5 ----- 2.5 TETRACYCLINE 8.6 9.8 7.2 11.2 TMP/SX 4.8 7.5 8.5 3.6 *ABCs Surveillance of Invasive MRSA + Fridkin SK, et al. NEJM 2005
2002 MRSA ISOLATES ATLANTACHARACTERISTICS – SCCmec TYPE SCCmec II SCCmec IV (n=142)(n=114) HA-MRSA 111 (78%) 14 (12%) CA-MRSA 24 (17%) 91 (79%) CULTURE SITE-SKIN 38 (27%) 83 (73%) USA100 136 (96%) 0 USA300 0 106 (93%) PVL 1 (0.7%) 111 (97%) CLIND-S, ERY-R 80 (56%) 110 (96%) POSITIVE D TEST 78 (98%) 7 (6%) Preliminary Report, CDC J. Hageman, et al.
EPIDEMIOLOGY CA-MRSA • FEW DATA DEFINING ISOLATES OR PREVALENCE IN HEALTHY SUBJECTS WITHOUT INFECTION OR PRESENTATION TO HCF • NATIONAL STUDY 5,000 HEALTHY US CITIZENS – 0.4% NASAL CARRIERS OF MRSA US-300 STRAINS (44TH ICAAC) • ASYMPTOMATIC MRSA COLONIZATION IN 5 DCC AND 3 KINDERGARTENS (TOKYO): 4.3% WITH 20/34 ISOLATES SCCmec TYPE II AND 14/34 ISOLATES SCCmec TYPE IV (5th INTERNATIONAL SYMPOSIUM ON ANTIMICROBIAL AGENTS AND RESISTANCE, APRIL 27-29, 2004) • NASHVILLE NASAL COLONIZATION MRSA 2001 IN HEALTHY CHILDREN 0.8% (PEDIATRIC STUDIES 0.2-2.2%); 2004 S. AUREUS 36.4% AND 2004 MRSA 9.2% CB Creech, et al. Pediatr Infect Dis J 2005; 24: 617-621
NATIONAL HEALTH AND NUTRITION EXAMINATION SURVEY (NHANES) U.S. 2001-2002 PREVALENCE STAPHYLOCOCCUSAUREUS NASAL COLONIZATION - PREVALENCE ESTIMATES 32.4% S. AUREUS / 0.8% MRSA; POPULATION ESTIMATES 89.4 MILLION PERSONS AND 2.3 MILLION PERSONS - HIGHEST S. AUREUS COLONIZATION 6-11 YEARS OLD 43-48% - YOUNGER AGE ISOLATES – SCCmec TYPE IV GENE MORE FREQUENT - PVL GENE IN 2.4% OF ISOLATES TESTED (8% OF MRSA) MJ Kuehnert, et al. J Infect Dis 2006; 193: 172-179
EPIDEMIOLOGY CA-MRSA • 84% OF SKIN INFECTIONS IN ILLINOIS ARE CURRENTLY CAUSED BY CA-MRSA (Robert Daum, M.D. Pediatric Academic Societies/Pediatric Infectious Diseases Society Annual Meeting, May 14-17, 2005 – Washington, DC) • TCH AUG 2001 – JUL 2004: COMMUNITY ACQUIRED S. AUREUS ISOALTES METHICILLIN R 71.5% TO 76.4% WITH GREATER RATE INCREASE CA-MRSA VS CA-MSSA (TOTAL # ISOLATES DOUBLED) - CA-MRSA ISOLATES, 95.6% OBTAINED FROM CHILDREN SKIN AND SOFT TISSUE INFECTIONS - 4.4% CHILDREN WITH INVASIVE INFECTIONS - ADMITTED TO HOSPITAL: 62% CA-MRSA; 53% CA-MSSA - CLINDAMYCIN R CA-MRSA 6%; CA-MSSA 11% • LE BONHEUR CHILDREN’S MED CENTER JAN 2000 – JUNE 2002: CA-MRSA 38% OF MRSA ISOLATES INCREASED TO 63% - EQUAL FREQUENCY STERILE SITE ISOLATES FOR CA-MRSA AND HCA-MRSA (16% VS 13%) - PFGE REVEALED 15/16 CA-MRSA ISOLATES USA 300 SL Kaplan, et al. Clin Infect Dis 2005; 40: 1785-1791 SC Buckingham, et al. Pediatr Infect Dis J. 2004; 23: 619-624
AUSTRALIAN EXPERIENCE WITH MRSA(COUNTRYWIDE DATA – “REPORTABLE DISEASE” • REPORTED CASES: 10 (1995) / 35,000 (2005) • CURRENT POPULATION-BASED RATE OF MRSA INFECTIONS: 250/100,000 • IN VITRO SENSITIVITY TESTING: OVER 97% STRAINS SENSITIVE TO TCN, TMP-SX, RIFAMPIN, CLINDAMYCIN • CLINDAMYCIN MOST FREQUENTLY USED ANTIBIOTIC (D-TEST DETECTED CA-MRSA INDUCEABLE RESISTANCE: VARIABLE WITH 2.2% TEXAS CHILDREN’S HOSPITAL/94% UNIVERSITY HOSPITAL, CHICAGO) KJ Christiansen. Management of community Staphulococcal infections in the era of community-acquired MRSA. Program and abstracts of the 45th Interscience Conference of Antimicrobial Agents and Chemotherapy; Dec 16-19, 2005; Washington, D.C. Abstract 1325
CA-MRSA MONCRIEF COMMUNITY HOSPITAL (FT. JACKSON, SC/12-18 INPATIENT BEDS/NO ICU) • % MRSA 1998-1999, 8-12%; 2000-2003, 23-32% (P<.01) • INPATIENT MRSA 1998-2000: 0-5 ISOLATES / YEAR • OUTPATIENT MRSA 1998-1999, 11-18/YEAR; 2000-2002, 32-53/YEAR (P<.01) • 2003 OUTPATIENT – CA-MRSA ANTIBIOTIC R PATTERN • MOST ISOLATES SCCmec IVa/PRODUCED PVL/PFGE TYPE USA 300 GJ Beilman. “Changing Epidemiology of gram-positive infections: CA-MRSA” 25th Annual Surgical Infection Society Meeting and Joint Surgical Infection Society Meeting of North America and Europe, May 5, 2005
EPIDEMIOLOGY CA-MRSA MILITARY MEDICAL TREATMENT FACILITIES (MMTF) • WRAMC, NNMC, USUHS (57 MMTF’S) 2001-2004: CLINDAMYCIN AND TMP-SX INCREASED 99% AND 62%, RESPECTIVELY - MRSA IN CHILDREN INCREASED FROM 6/138 TO 60/215 ISOLATES (P<0.001); IN ADULTS 161/715 TO 324/972 ISOLATES (P<0.001) - CLINDAMYCIN R INCREASED S. AUREUS ISOLATES FROM 1/207 TO 13/327 (P<0.05) • BROOKE ARMY MEDICAL CENTER AUG 25 – DEC 18, 2003 HEALTH CARE SPECIALIST COURSE, FIRST 8-10 WEEKS OUTSIDE HEALTH CARE ENVIRONMENT (812 SOLDIERS) - INITIAL SAMPLING 24 SOLDIERS (3%) COLONIZED WITH CA-MRSA WITH 9 (38%) DEVELOPING SOFT-TISSUE INFECTION - INITIAL SAMPLING 229 SOLDIERS (28%) COLONIZED WITH MSSA WITH 8 (3%) DEVELOPING CLINICAL INFECTION - FOLLOW-UP CULTURE WITH 1.6% COLONIZATION RATE - PREVIOUS ANTIBIOTIC USE RISK FACTOR FOR CA-MRSA COLONIZATION WITH INITIAL SAMPLING (P=0.03) - PVL GENES IN 66% OF 45 RECOVERED CA-MRSA ISOLATES - ALL 9 CLINICAL ISOLATES WITH PVL GENES; 6 OF SOLDIERS HOSPITALIZED 5/6 PVL POSITIVE CA-MRSA INFECTIONS - CA-MRSA COLONIZATION WITH PVL-POSITVE STRAINS WAS ASSOCIATED WITH SIGNIFCANT RISK SOFT-TISSUE INFECTIONS – SUGGESTS CA-MRSA MORE VIRULENT THAN MSSA L. Braun, et al. Pediatr Infect Dis J 2005; 24: 622-626 MW Ellis, et al. Clin Infect Dis 2004; 39 : 971-979
CA-MRSA OUTBREAKS IN WELL-DEFINED POPULATIONS & SPECIFIC SETTINGS • CHILDREN (INCLUDING NEONATES), IVDU, MSM • NATIVE AMERICANS • PACIFIC ISLANDERS • CORRECTIONAL FACILITY INMATES • COMPETITIVE SPORTS PARTICIPANTS • HIV INFECTED ADULTS • MILITARY PERSONNEL • 2003-2004 INFLUENZA SEASON JT Weber, Clinical Infectious Diseases 2005: 41: S269-272 C. Matthews, et al. J Acquir Immune Defic Syndr 2005; 40: 155-160
MICROBIOLOGY • WITH NEWER MOLECULAR TECHNOLOGIES, RAPID DETECTION mecA GENE IS POSSIBLE • TO OPTIMIZE TREATMENT, ANTIMICROBIAL SUSCEPTIBILITY PATTERNS OF CA-MRSA CRUCIAL WITH PHYSICIANS ENCOURAGED TO OBTAIN PURULENT SPECIMEN CULTURES TO DETERMINE PROPORTION MRSA AMONG CA - S. AUREUS • VANCOMYCIN, TMP-SX, CLINDAMYCIN, DOXYCYCLINE, AND LINEZOLID INCLUDED IN ROUTINE PANEL OF AGENTS TESTED • DETECTING INDUCIBLE MACROLIDE-LINCOSAMIDE-STREPTOGRAMIN B IS RECOMMENDED WHEN CLINDAMYICN IS AN IMPORTANT TREATMENT OPTION (R 4-6% TO 20% IS SOME REGIONS)
MLS (INDUCIBLE CLINDAMYCIN) RESISTANCE MECHANISMGENEERYTHROMYCINCLINDAMYCIN EFFLUX msrARS RIBOSOMAL (constitutive) ALTERATION ermRR RIBOSOMAL (inducible) RS (on initial testing) ALTERATIONerm i MLSB PHENOTYPE R (when exp. to erythr.) ** NOT RECOMMENDED TO USE CLINDAMYCIN TO TREAT MRSA INFECTIONS UNLESS THE APPROPRIATE D-TEST FOR iMLSB RESISTANCE IS CONDUCTED ON ISOLATE (GUIDELINES OF THE CLINICAL & LABORATORY STANDARDS INSTITUTE)
MLS ResistanceThe D test • MLS resistance can not be detected by: • Standard broth microdilution testing • Automated susceptibility testing devices • Standard disk diffusion test • E-test http://www.phppo.cdc.gov/nltn/pdf/2004/2_Hindler_D-Test.pdf
INDUCIBLE CLINDAMYCIN R. IN STAPHYLOCOCCI: SHOULD CLINICIANS AND MICROBIOLOGISTS BE CONCERNED? • DATA FROM REPORTS USING CLINDAMYCIN TO TREAT S. AUREUS INFECTION WITH INDUCIBLE MACROLIDE, LINCOSOMIDE, AND GROUP B STREPTOGRAMIN R (MLSBi) PHENOTYPE • OF 11 PATIENTS, 8 FAILURES INCLUDING 4 RELAPSES JS Lewis and JH Jorgensen. Clin Infect Dis 2005; 40: 280-285
CA-MRSA PREDOMINANTLY CAUSES SKIN DISEASE DISEASE SYNDROME(%) • SKIN/SOFT TISSUE 90-95% - FOLLICULITIS, PUSTULAR LESIONS, FURUNCLES/CARBUNCLES/ABSCESSES - RAPIDLY PROGRESSIVE CELLULITIS (DISTINCTIVE) • ENT – OTITIS MEDIA (PET’S), SINUSITIS, MASTOIDITIS • INVASIVE INFECTIONS 5-10% - SEVERAL INVASIVE CA-MRSA SYNDROMES DESERVE SPECIAL ATTENTION, APPEARING NOVEL OR ATLEAST NOT FOUND IN RECENT LITERATURE JK Todd. Pediatrics in Review 2005; 26: 438-443
COMMUNITY-ACQUIRED S. AUREUS INFECTIONS AT TEXAS CHILDREN’S HOSPITAL (AUG 1, 2001 – JULY 31, 2004) TOTAL CA INFECTIONS (#3,586) MRSA (#2,661) MSSA (#925) SYSTEMIC SKIN & SOFT TISSUE SYSTEMIC SKIN & SOFT TISSUE (110) (2,551) (71) (854) INPATIENT OUTPATIENT INPATIENT OUTPATIENT (1,579) (972) (456) (397) P=0.00002 SL Kaplan, et al. Clin Infect Dis 2005; 40: 1785-1791
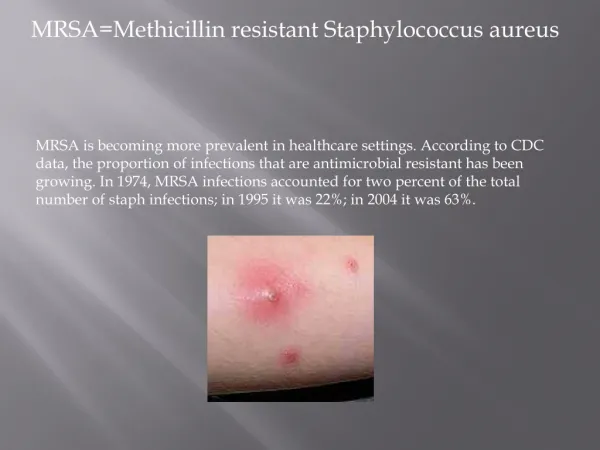
Examples of CA-MRSA Skin Infections Infections with CA-MRSA may be confused with spider bites, impetigo, varicella
SECULAR TRENDS IN SSTI RATES • MORE SSTIs AS WELL AS INCREASE IN MRSA SSTIs • #11 COORDINATING SITES, CDC’S EMERGEncy ID NET - PREVALENCE OF MRSA AS CAUSE OF SSTI IN ADULT ED PATIENTS: 59%; 98% PVL+; 97% USA300; 72% USA300-0114 - EMERGEncy ID NET, MORAN GJ, ET AL. SAEM 2005 & RACHEL GORWITZ, CDC • 1992 TO 2003 NATIONAL HOSPITAL AMBULATORY MEDICAL CARE SURVEY (SSTI VISITS TO US ED’S / 1,000 US POPULATION) - 1992-1992, 3.75-5; 2002-2003, 5.25-8.0 - PITT & STEINBERG ID5A 2005
CA-MRSA CLINICAL MANIFESTATIONSSKIN & SOFT TISSUE INFECTIONS • CONSTITUTE GREATER THAN 90% OF INFECTIONS IN CHILDREN • PREDOMINANTLY CELLULITIS, FOLLICULITIS, ABSCESSES (“BOILS”) • SOME SKIN ABSCESSES ARE LOCALLY DESTRUCTIVE INCLUDING INITIAL PAINFUL PAPULE THAT BECOMES PURULENT & NECROTIC – “SPIDER/INSECT BITE” (DL Swanson & RS Vetter: Bites of brown recluse spiders and suspected necrotic arachnidism. N Engl J Med 2005; 352: 700) • RECURRENT SKIN INFECTIONS SEEN FREQUENTLY AND CLOSE CONTACTS WITH SIMILAR SKIN INFECTIONS (MC Lee, et al. Pediatr Infect Dis J 2004; 23: 123 / CDC: MRSA infections among competitive sports participants – Colorado, Indiana, Pennsylvania, Los Angeles County, 2002-2003. MMWR Aug 22, 2003; 52(33): 793) • HEAD AND NECK CA-MRSA INFECTIONS – CERVICAL, LYMPHADENITIS, OTITIS EXTERNA, OTITIS MEDIA WITH OTORRHEA, ACUTE MASTOIDITIS, SINUSITIS (FAB Santos, et al. Arch Otolaryngol Head Neck Surgery 2000; 126: 1383-1385) • SEPSIS IS ATYPICAL • MOST CA-MRSA CARRY pvl GENES ENCODING FOR CYTOTOXIN PANTON-VALENTINE LEUKOCIDIN – IMPLICATED FACTOR OF POSSIBLE ENHANCED ABILITY OF CA-MRSA CAUSING SKIN INFECTIONS(F Vandenesch, et al. Emerg Infect Dis 2003; 9: 978-984 / AMA Mishaan, et al. Pediatr Infect Dis J 2005; 24: 201-206) SL Kaplan, et al. Clin Infect Dis 2005; 40: 1785-1791 SK Fridkin, et al. N Engl J Med 2005; 352: 1436-1444 BC Herold, et al. JAMA 1998; 279: 593-598 TS Naimi, et al. Clin Infect Dis 2001; 33: 990-996
CA-MRSA AMONG HEALTHY NEWBORNS • CHICAGO - 11 CASES WITH PUSTULAR-VESICULAR LESIONS - C-SECTION 82%; 82% MALE; AGE AT ONSET MEDIAN 7 DAYS - ONE PHYSICIAN / ONE NURSA MRSA NASAL CARRIAGE - 8 ISOLATES TESTED: ALL USA300; (7/8 USA300 – 0114); ALL PVL + • LOS ANGELES - 11 CASES WITH PUSTULAR-VESICULAR LESIONS IN GROIN - C-SECTION 64%; 100% MALE; MEDIAN NURSERY STAY 4 DAYS - 7 ISOLATES CHARACTERIZED – ALL USA300 – 0114 MMWR March 2006
CA-MRSA INVASIVE INFECTIONS • OSTEOMYELITIS – MULTIPLE SITES, DEEP VENOUS THROMBOSIS • PNEUMONIA WITH/WITHOUT EMPYEMA – INCLUDING NECROTIZING PNEUMONIA WITH/WITHOUT PLEURAL EMPYEMA WITH DESTRUCTIVE PNEUMONITIS WITH LOSS OF PULMONARY ARCHITECTURE, MICROABSCESSES, AND PULMONARY VASCULITIS • SEPTIC ARTHRITIS/BURSITIS • PYOMYOSITIS/MYOSITIS/NECROTIZING FASCIITIS • LYMPHADENITIS • MUSCULOSKELETAL INFECTION AND DEEP VEIN THROMBOSIS (FEW PEDIATRIC CASES IN LITERATURE) • BACTEREMIA/SEPTICEMIA – INCLUDING A NEW AND DEVASTATING PURPURA FULMINANS SYNDROME; WATERHOUSE – FRIDERICHSEN SYNDROME • DEEP ABSCESSES – EPIDURAL, LUNG, RENAL, PARASPINAL, SACRAL • TOXIC SHOCK SYNDROME
TCH HOSPITAL COURSE & OUTCOME WITH INVASIVE CA-MRSA & CA-MSSA OUTCOMEMRSA(N46)MSSA(N53)P CURE/IMPROVEMENT 45 52 NS DEATH 1 1 FEBRILE DAYS - MEAN+SD 3.93+4.12 1.8+1.69 0.07 - MEDIAN 3 (0-14) 2 (0-6) HOSPITAL DAYS - MEAN+SD 12.02+7.64 9.02+8.54 0.005 - MEDIAN 9 (3-37) 7 (0-44) PICU DAYS - MEAN+SD 6.6+4.75 9+4.3 0.49 - MEDIAN 9 (1-15) 7 (6-14) DAYS OF BC+ 15 PATIENT 18 PATIENTS - MEAN+SD 2.87+2.45 1.5+1.04 0.084 - MEDIAN 1 (1-8) 1 (1-4) G Martinez, et al. Pediatr Infect Dis J 2003