Download
1 / 18
190 likes | 527 Views
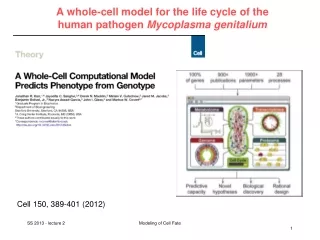
Mycoplasma genitalium. Carina Bjartling Dep of Gyn & Obst Skane University Hospital, Malmö, Sweden. Mycoplasmas - class mollicutes. Free-living small bacteria (0.3 - 0.5 μm) Lack a rigid cell wall Commonly found in the human urogenital tract: - M. genitalium 580 bp (1-3%)

E N D
Mycoplasma genitalium Carina Bjartling Dep of Gyn & Obst Skane University Hospital, Malmö, Sweden
Mycoplasmas-class mollicutes • Free-living small bacteria (0.3 - 0.5 μm) • Lack a rigid cell wall • Commonly found in the human urogenital tract: - M. genitalium 580 bp (1-3%) - M.Hominis 665 bp (20-50%) - Ureaplasma urealyticum 840-950 kbp andU. parvum 751 kbp (40-80%)
Urogenital mycoplasmas Jensen and Unemo. WHO Manual. 2013
Urogenital mycoplasmas • M.hominis, U.urealyticum, U.parvum- commonly detected in healthy individuals • Their association with urogenital infection in either men or women remains to be conclusively proven
Mycoplasma genitalium • Well documented as an agent of NGU in men • Sexually transmitted • Documented as an agent of cervicitis in women • Less well documented in PID • Limited documentation as a patogen in ectopic pregnacy and TFI • Scarse documentation as a patogen in adverse obstetrical outcome
Mycoplasma genitalium • Documented association with HIV and recently a study showing M.genitalium infection to facilitate acquisition of HIV-1 (Mavedzenge SN et al, 2012) • SARA- case reports but no systematic studies
Prevalences of M.genitalium Estimated prevalences in 40 independent studies (27000 women) screened for M.genitalium world wide: - 7.3 % in high-risk population (0 – 42%) - 2.0 % in low-risk population (1- 5 %) - CT (4.2 %) and Ng (0.4 %) (USA) (McGowin et al, 2011) Prevalence in Malmö, Sweden at the women’s clinic emergency service between 2003-2008 in 5519 women -MG- 2.1 % -CT- 2.8 % (Bjartling et al, 2012)
Clinical studies of M.genitalium and PID Case –control studies: Uno et al. 1997, Japan. 2/49 (4%) in cases, 0/80 (0%) in controls Cohen et al. 2002, Kenya, Nairobi. 9/58 (16%) in cases, 1/57 (2%) in controls, endometrial specimen Simms et al. 2003, UK. 6/45 (13%) in cases, 0/37 (0%) in controls Cohen et al. 2005, Kenya, Nairobi. 9/123 (7%), abd. fluid- 1/123 (1%), Haggerty et al. 2006, USA. 7/50 (14%),(8% in endometrial specimen) Bjartling et al. 2012, Sweden. 4/81 (4.9%) in cases, 2/346 (0.6%) in controls Prospective studies: Oakeshott et al, 2010, UK. 3/77 (4%), 12 months follow up Bjartling et al. 2010, Sweden, 6/49 (12%) in cases, 4/168 (2%) in controls, post abortal PID, 6 weeks follow up
Proportions of M.genitalium and C.trachomatis attributable to PID M.genitalium - 4- 16% (5 studies, 1997- 2012) C.trachomatis - 20- 55% (19 studies through the 1990s) - 42% (POPI trial, 2004-2007)
Serological studies of M. genitalium, PID, TFI and ectopic pregnancy – Möller et al, 1984, UK. MG – ab in 40 % of 31 women with PID Lind et al, 1987, Denmark. No ass. between MG – ab and PID in 95 cases of salpingitis Clausen et al, 2001, Denmark, MG- ab in 22 % (29/132) TFI compared to 6.3 % (11/176) of the controls Jurstrand et al, 2007, Sweden, no sign. difference between MG –ab in PID, ectopic pregnancy and normal controls Svenstrup et al, 2008, Denmark. MG – ab in 17 % of 30 TFI cases compared to 4% of the controls Stephen et al, 2006, USA. 2.5 times higher infertility rate among women with MG in the endometrium . Register study 1982-2002
M.genitalium and adverse obstetric outcome • Oakeshott et al 2004, UK, 1216 early pregnant, no ass with miscarriage , MG prevalence 0.7 % • Labbe et al 2002, no sign ass with preterm delivery • Kataoka et al, 2006, no ass for preterm delivery • Edwards et al 2006, USA, Florida. 134 pregnant women, prospective study, preterm delivery, OR 3.48 (1.41- 8.57). • Hitti et al 2010, ass with preterm delivery,OR 2.5 (1.2-5.0)
Diagnosis of M.genitalium • Culture is insensitive and extremely slow • Serologi has low specificity and low sensitivity • NAAT is the only practical method for diagnosis - technically demanding, organism load 100-fold lower than C.trachomatis • No validated (FDA), commercially available assays • Important to validate and quality assure in-house assays • Real- time PCR- robust and lower risk of contamination than PCR
Genital specimen for diagnosis of M.genitalium Summary Men: - FVU (67.0- 97.6%) - Urethral swab (58.0- 82.5%), Women: - self collected vaginal swab (91.0%) - clinician collected cervical swab (58.9- 74.3%) - clinician collected vag swab (57.0- 72.6%) - FVU (61.4- 88.0%) Jensen JS et al, 2004 Wroblevski JK, 2006 Jurstrand M et al, 2005 Edberg A et al 2009 Shipitsyna E, 2009 Lillis RA, 2011 Mobley et al 2012
Treatment of M.genitalium infections • Cure rates of different antibiotics are relatively low and declining • Cure rate azithromycin (1 g azithromycin): • Settings with high usage of azithromycin: 40-85% • Settings with low usage of azithromycin: 95-100%? • Cure rate doxycycline: • 17-45% • Cure rate fluoroquinolones: • Ofloxacin: 50% • Moxifloxacin: 100% Falk, et al. STI. 2003Jernberg, et al. IJSA. 2008Bjørnelius, et al. STI. 2008Mena, et al. CID. 2009Terada, et al. JIC. 2011 Twin, et al. PLoS. 2012Manhart, et al. CID. 2013
Treatment of M.genitalium infections First choice: - Azithromycin 500 mg×1 day 1 + 250 mg×1 in the 4 following days (ideally, test-of-cure in ≥14 days) Second choice (if treatment failure and not as first choice!)- Moxifloxacin 400 mg×1 daily in 7 days Jensen, personal communication, July 2013
Take home messages • The estimated proportion of M.genitalium and C.trachomatis attributable to PID is about 2-16% and 20-55% respectively • Focus on detection and treatment of M.genitalium (not M.Hominis or Ureaplasma spp) • Important to validate and quality assure in-house assays • No clear guidance can be given in the choice of optimal genital specimen but FVU in men and self collected vaginal specimen in women seems to have the highest bacterial load • Cure rates of different antibiotics are relatively low and antimicrobial resistance and treatment failure in M.genitalium infections are common • First choice for treament of M.genitalium infection is Azithromycin 500 mg×1 day 1 + 250 mg×1 in the 4 following days