Download
1 / 26
260 likes | 448 Views
Step by Step –working with children who inject drugs : A tool for building the capacity of organisations . Bikash Gurung, Youth RISE Anita Krug, Youth RISE Maria Phelan, Harm Reduction International Vanessa Veronese, Save the Children Kate Iorpenda, International HIV AIDS Alliance

E N D
Step by Step –working with children who inject drugs :A tool for building the capacity of organisations • Bikash Gurung, Youth RISE • Anita Krug, Youth RISE • Maria Phelan, Harm Reduction International • Vanessa Veronese, Save the Children • Kate Iorpenda, International HIV AIDS Alliance • Scott McGill, Save the Children • WEWSO1 Skills Building Workshop AIDS 2014 Melbourne, Australia July 22nd
The young person’s experience accessing harm reduction services (picture) Results of Youth RISE Global Community Consultations
The consultations • Conducted in 14 countries; • 132 participants • Focus on • Barriers to accessing the comprehensive package of harm reduction services • Recommendations for improved access and additional support from the perspective of young people who use drugs
Findings • Barriers to services: • No knowledge of existence of services • ‘When you are young, you don't know where to turn for help. You don't know Stigma [needle and syringe programme in Ljubljana] exists. Lack of information is the biggest problem when you are young. You don't know where to turn for syringes. We were looking for them in random cars’ (Young man, Slovenia) • Age restrictions/parental consent requirements • 'First of all they will not go to NSPs because they are minors and they need to come with someone from the family, the majority don’t want their family to know’ (Young woman, Romania) • Do not feel they need services; believe drug services are for older, heavily drug dependent users • ‘We don’t need services. We have no problems’.
Findings Cont. • Fear of police harassment • Lack of ‘youth-friendly’ services • Bullied by older users • Staff attitudes • Prefer pharmacies which are more discreet • Need for comfortable, non-judgemental environment • ‘We want a safe place with a warm response and a happy face’ (Young man, Indonesia) • ‘A place to visit without any fear with staff that care about your soul’ (Young woman, Ukraine)
Global Data Snapshot • A global population size estimate for people who inject drugs under the age of 18 is unavailable • The contribution of injecting among under-18s to HIV epidemics is largely unknown. • National population size estimates are exceptionally rare and age disaggregation in HIV surveillance is poor.
Ukraine: No. of adolescents who inject drugs versus access to harm reduction services through the International HIV AIDS Alliance See: O. Balakireva et al Population Size Estimate of Most-At-Risk Children and Youth in the 10–19 Age Group, Kyiv: Unicef, 2011 and D. Barrett, N. Hunt and C. Stoicescu Injecting drug use among under 18s: A snapshot of available data, London: Harm Reduction International 2013.
Available studies show… • Low ages of initiation across regions. • In some countries significant proportions of people who inject drugs are adolescents (e.g. Nepal, 20%) • Important differences between younger people who inject drugs and older counterparts, including in risk-taking behaviour and access to services • Specific groups of young people are at increased risk, in particular those who are street involved • Significant variations between countries and within them (picture)
Indonesia: % people who inject reporting needle sharing disaggregated by age • See: National AIDS Commission (2011) Report: Age group disaggregation of survey and research data. Jakarta: KPA
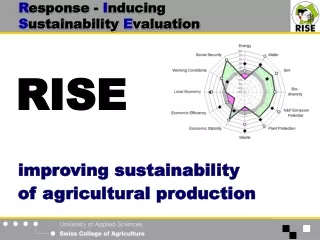
Context is key: To what extent are good practices transferable?
Exercise Scenario 1 You are working in a needle-syringe program. Most of your clients are 20-40 years old. One day, a 12-year-old girl comes in and asks for injecting equipment. At first, you are simply surprised (or amazed). After some discussion, it becomes clear that the girl is an active injector. Should you provide her with injecting equipment? Is it ethical, the right thing, to give injecting equipment to a young person? Is your service a suitable place for such a young person and prepared for work with her? Does the potential harm to the girl from using unsterile equipment outweigh any potential harms from providing her with injecting equipment? Can this person provide the consent necessary for this form of assistance? Scenario 2 You are working with street children with many significant problems. One day, you meet a 14-year-old boy who is obviously a drug user. As a well-trained youth worker, you know the local referral network and you know that no agencies – drug treatment, HIV prevention – will provide services to a drug user aged fewer than 18. What are your options? Do you simply say that nothing can be done? Do you provide assistance that you pay for yourself – against your organisation’s policy? Do you advocate for changes to national policies – knowing that these changes may take years to come into effect?
Scenario 3 • You are working in a HIV testing centre, providing counselling and HIV testing. A 15-year-old girl receives a positive HIV test result. In post-test counselling discussions, she says her greatest risk factor is injecting drugs with her 16-year-old boyfriend. They usually inject in a group of 10-12 friends and often share needles and syringes. It is illegal in your country to provide harm reduction services to anyone aged under 18. • What are your options? • What are the potential risks? • What action would you take? Scenario 4 You are conducting outreach and you come across a young group of people who inject drugs. While you and your colleagues are talking to the group, you notice one of the young girls has a black eye. You speak to her and she tells you that she lives with her uncle, who regularly abuses her. • What is your duty of care to this girl? • What steps would you take? • What additional information would you need to find out from the girl?
An introduction to the tool and preliminary results of a three-country pilot study • Background: • Global meta review, 2012: No guidance for service providers on specific challenges of working with children who inject drugs • Importance of making sure organisations are well prepared to deal with these challenges • ‘Proactive vs Reactive’ approach to working with children
What is Step by Step? • 10 Steps to help service providers address ethical, legal and practical dilemmas of working with children and adolescents • Goes beyond youth friendly services; meeting child safeguarding and protection obligations, addressing wider, non-HR harms
Content Step 1: Exploring attitudes and sharing concerns Step 2: Assessing and understanding policy and legal environment Step 3: Understanding key principles for working with children Step 4: Exploring your current capacity to work with children who inject drugs Step 5: Assessing the needs of children who inject drugs Step 6: Determining your capacity to provide key services Step 7: Mapping other available services Step 8: Considering the impact on staff Step 9: Policies to assist children who inject drugs Step 10: Developing your policy
Step by Step service delivery pilot testing • Nepal, Romania and Kenya • Aimed at service providers and those working in the field • Three stage pilot process: • 1. Pre-pilot questionnaire • 2. Post-Step Survey • 3. Post-pilot questionnaire
Preliminary Pre-pilot findingsNepal I am comfortable providing <18 to other service providers I understand <18 and >18 have different needs I have a good understanding of CP principles I know what 'child-friendly' services mean
Preliminary Pre-pilot findingsNepal I think our organisation has a very clear CP policy My colleagues know what to do if they encounter a <18 during outreach I am comfortable giving an <18 a clean needle I cannot provide HR services to <18
What have we learned? • Need for ‘champions’ within organisation • Need to also target project developers • Concepts of ‘child protection’, ‘evolving capacities’ are not articulated as such, but understood informally
What next? • Finalisation • Dissemination strategy • Register your interest!
Exercise: • A teenage girl has approached your mobile outreach workers asking for needles, syringes and condoms, she is thin and her clothes are dirty. While talking to her she • explains she regularly injects and most of the time she sleeps on the street as there is too much fighting at • home. • Your organisation is not officially allowed to give anyone under 18 services unless there is parental consent
Fraser Guidelines 1. Does the young person understand what is being provided or suggested, and the rationale for the products/ service? 2. Does the young person refuse to provide parental consent? 3. Is the young person likely to continue risky behaviour or to remain in a risky environment? 4. Is the young person’s physical or mental health likely to suffer if the products/ services or not provided? 5. Are the young person’s best interests served by providing the products/ services?
Exercise J: Determining priority services for children who inject drugs Exercise K: Comparing service need with what is available Exercise C: Mapping the legal environment Exercise B: TRUE / FALSE exercise: Attitudes to common dilemmas Exercise D: Weighing the risks vs. benefits when deciding to provide services to children who inject drugs Exercise E: Who knows best?
Using the Step by Step Tool How would this tool help service providers in your country context to address ethical, legal and practical dilemmas of working with children and adolescents who inject drugs? What improvements, suggestions or changes would you like to suggest? Other comments?