Download
1 / 21
210 likes | 377 Views
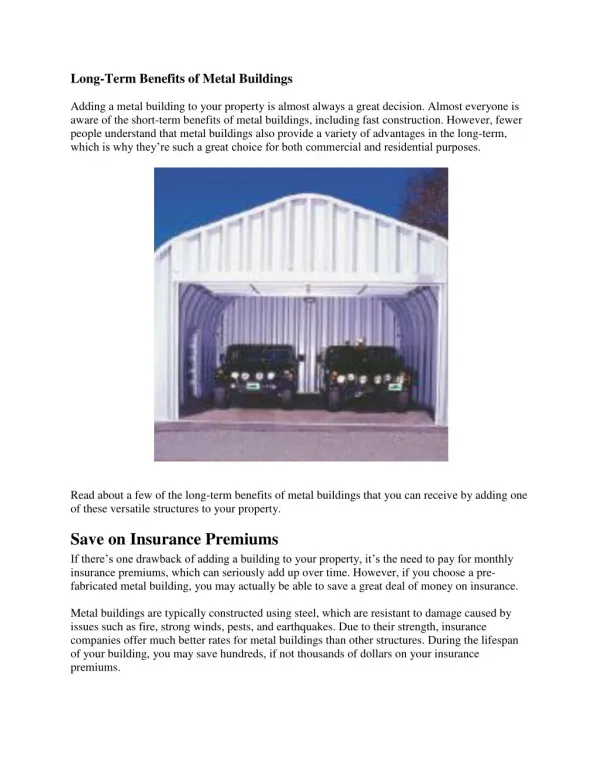
LONG TERM BENEFITS OF ORAL AGENTS. J. Robin Conway M.D. Diabetes Clinic Smiths Falls, ON www.diabetesclinic.ca. Long Term Benefits of Oral Agents. Robin Conway M.D. Physical Activity and Diabetes.

E N D
LONG TERM BENEFITS OF ORAL AGENTS J. Robin Conway M.D. Diabetes Clinic Smiths Falls, ON www.diabetesclinic.ca
Long Term Benefits of Oral Agents Robin Conway M.D.
Physical Activity and Diabetes • For people who have not previously exercised regularly and are at risk of CVD, an ECG stress test should be considered prior to starting an exercise program Testing is particularly important before, during and for many hours after exercise.
Nutrition Therapy People with diabetes should: • Receive nutrition counseling by a registered dietitian • Receive individualized meal planning • Follow Canada’s Guidelines for Healthy Eating • People on intensive insulin should also be taught to adjust the insulin for the amount of carbohydrate consumed
Pharmacologic Management of Type 2 Diabetes • Add anti-hyperglycemic agents if: Diet & exercise therapy do not achieve targets after 2-3 month trial or newly diagnosed and has an A1C of 9% Intensify to reach targets in 6-12 months
Clinical assessment and initiation of nutrition therapy and physical activity Mild to moderate hyperglycemia (A1C<9.0%) Marked hyperglycemia (A1C 9.0%) Overweight Non-overweight 2 antihyperglycemic agents from different classes Basal and/or preprandial insulin Biguanide alone or in combination 1 or 2 antihyperglycemic agents from different classes If not at target If not at target If not at target If not at target Add an oral antihyperglycemic agent from a different class or insulin Intensify insulin regimen or add antihyperglycemic agents Add a drug from a different class or use insulin alone or in combination Management of Hyperglycemia in Type 2 Diabetes Patients
Oral Agents for Type 2 Diabetes • Combination at less than maximal doses result in more rapid improvement of blood glucose • Counsel patients about hypoglycemia prevention and treatment SMBG is recommended at least once daily
Targets for Glycemic Control * Treatment goals and strategies must be tailored to the patient, with consideration given to individual risk factors To achieve an A1C 7.0%, patients should aim for FPG, preprandial and postprandial PG targets
Burden of Poor Control - Cost • Estimate annual cost to health plans by level of glycemic control • Determine effect of Improved Glycemic Control on Health Care Utilization and Costs
Oral Antihyperglycemic Agents: Biguanides • Decreases hepatic glucoseproduction, enhances peripheral glucose uptake • May reduce insulin resistance in the periphery • e.g., Metformin • Contraindicated in renal/hepatic insufficiency • May cause GI side effects • Not associated with hypoglycemia, may promote weight loss LIVER MUSCLE Meltzer et al CMAJ 1998;159(Suppl):S1-29.
Oral Antihyperglycemic Agents: Thiazolidinediones (TZDs) • Decrease insulinresistance • Increase insulin-dependent glucose disposal, decrease hepatic glucose production • e.g., Pioglitazone, rosiglitazone • Pioglitazone has a positive effect on lipids • Not associated with hypoglycemia • Possible URI, headache, edema, weight gain and reduction in hemoglobin MUSCLE LIVER ADIPOSE TISSUE Plosker, Faulds Drugs 1999;57:410-32. Balfour, Plosker Drugs 1999;57:921-30.
TZD TZD Thiazolidinediones: Mechanism of Insulin Sensitization INSULIN INSULIN RECEPTOR GLUCOSE GLUT-4 PPAR DNA RNA Saltiel, Olefsky Diabetes 1996;45:1661–9.
Durability of Glycemic Control with Pioglitazone Long Term HbA1c (%) Einhorn D et al. Diabetes 2001;50 (suppl2):A111
Metformin & Pioglitazone Study - Open Label Extension Change in HbA1c (%) Change in fasting glucose (mmol/L) Einhorn et al. Clin Therapeutics 2000;12:1395-1409
Oral Antihyperglycemic Agents: Sulfonylureas • Stimulate pancreatic insulin release • e.g., First-generation: tolbutamide, chlorpropamide, acetohexamide • e.g., Second-generation: Glyburide, gliclazide • Secondary failure a problem • Weight gain, risk of hypoglycemia PANCREAS Meltzer et al CMAJ 1998;159(Suppl):S1-29.
Natural History of Type 2 Diabetes Henry. Am J Med 1998;105(1A):20S-6S.
Oral Antihyperglycemic Agents: Alpha-glucosidase inhibitors • Slows gut absorptionof starch and sucrose • Attenuates postprandial increases in blood glucose levels • e.g., Acarbose • GI side effects • Not associated with hypoglycemia or weight gain INTESTINE Salvatore, Giugliano Clin Pharmacokinet 1996;30:94-106.
Oral Agents for Type 2 Diabetes • Combination at less than maximal doses result in more rapid improvement of blood glucose • Counsel patients about hypoglycemia prevention and treatment SMBG is recommended at least once daily
Insulin Natural History of Type 2 Diabetes Metformin/Thiazolidinediones Secretagogues Lifestyle Henry. Am J Med 1998;105(1A):20S-6S.
Targets for Glycemic Control * Treatment goals and strategies must be tailored to the patient, with consideration given to individual risk factors To achieve an A1C 7.0%, patients should aim for FPG, preprandial and postprandial PG targets