Download
1 / 14
140 likes | 149 Views
A 69-year-old Caucasian male with no prior renal history except hypertension presented with respiratory failure and hemoptysis. Imaging and tests revealed ground glass opacification in all lobes of the lungs. Renal biopsy showed crescentic glomerulonephritis in a late stage with extensive glomerulosclerosis and parenchymal atrophy. Immunofluorescence suggested an immune complex etiology, but electron microscopy indicated a pauci-immune background.

E N D
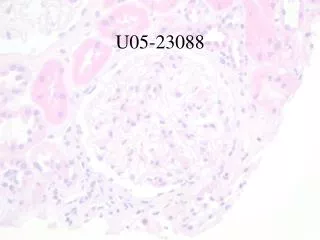
U05-16925 • 69 yo Caucasian male; no prior renal history except HTN • presented with respiratory failure and hemoptysis; CXR and HRCT revealed ground glass opacification in all lobes (L>R) with no evidence of PE; BAL negative for infection • no rash, no ENT/eye symptoms, no oral ulcers • recent DVT of R leg diagnosed ~22/8/05 • admission creatinine 5 Sept 2005 was 462 uM; u/a 3+ blood, 3+ protein, hemegranular casts, rare RBC cast; protein/creatinine ratio=113 mg/mmol • 22 August 2005 creatinine = 226 uM • December 2004: creatinine 97 uM, u/a 1+ blood, 2+ protein (no quantitation) • November 2002: creatinine 93 uM, u/a 3+ blood, trace protein, SG 1.030 • serology positive for p-ANCA, ANA (fine speckled, centromere negative), and rheumatoid factor (78, N<20); normal complements • RENAL BIOPSY 7 Sept 2005
Immunofluorescence • IgG – Trivial to mild mesangial staining • IgA – Mild mesangial staining • IgM – Mild mesangial staining, mild vascular staining • C3 – Moderate to strong vascular staining, Moderate mesangial staining • C1q – Negative • Kappa – Trivial to mild mesangial staining • Lambda – Trivial to mild mesangial staining • Fibrinogen – Moderate interstitial staining. Strong staining of glomerular crescents • Albumin – Negative
Diagnosis: • Crescentric Glomerulonephritis in a late stage with extensive glomerulosclerosis and parenchymal atrophy and scarring • Immunofluorescence suggests an immune complex etiology but electron microscopy is compatible with a pauci-mmune background