Download
1 / 39
480 likes | 815 Views
Melanoma. Hai Ho, M.D. Department of Family Practice. Epidemiology. Sixth most common cancer Incidence increases from 1/1500 in 1930 to 1/75 in 2000 1% of skin cancer but account for 60% of skin cancer death. Risk factors?. Sun exposure Intermittent intense exposure Childhood

E N D
Melanoma Hai Ho, M.D. Department of Family Practice
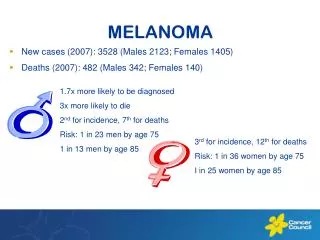
Epidemiology • Sixth most common cancer • Incidence increases from 1/1500 in 1930 to 1/75 in 2000 • 1% of skin cancer but account for 60% of skin cancer death
Risk factors? • Sun exposure • Intermittent intense exposure • Childhood • UVB > UVA – higher incidence near equator • Tanning bed
Clinical prediction rule American Cancer Society’s ABCDE
D Melanoma could occur in lesions less than 6 mm
E Elevation or Enlargement by patient report
Sensitivity of ABCDE rule If melanoma truly exists, the rule will detect it 92-97% (average 93%) of the time, when one criterion is met
Caution • If none of the criteria is met, 99.8% chance that the lesion is not a melanoma (high negative predictive value) • May miss amelanotic melanomas and melanomas changing in size
Growth patterns • Radial growth • Lasts for months to years • Growth and regression due to restraint by immunologic system • Horizontal and vertical growth • More poorly differentiated • Produce nodule or mass
Superficial spreading melanoma White = regression • 50% of melanoma cases • Common in middle age • Radial spread and regression
Nodular melanoma • 20-25% of melanoma cases • Common in 5-6th decade • Vertical growth and no horizontal growth phase
Lentigo maligna melanoma Lentigo maligna Lentigo maligna melanoma • 15% of melanoma cases • Elderly – 6-7th decade • Lentigo maligna • Horizontal growth phase for years • Bizarre shapes from years of growth and regression • Transform to lentigo maligna melanoma
Acral-lentigious melanoma • 10% of melanoma cases • In palms, soles, terminal phalanges, and mucous membrane • Growth phase similar to lentigo maligna and lentigo maligna melanoma • Aggressive tumor and early metastasis
Excisional biopsy Preferred method – deepest level of penetration for staging
Punch biopsy Stretch the skin perpendicular to the skin line Subcutaneous fats Wound <4mm may not be sutured
Shaving Never because prognosis and treatment are based on the level and depth of invasion
Pathology • Depth of invasion • Growth pattern (nodular, superficial spreading, etc.) • Margin status • Presence or absence of ulceration
Depth of invasion • Breslow • Measure the actual thickness • More reproducible and accurate in determining prognosis • Clark • Report by anatomical site • Significant if tumor ≥ 1mm
Indications for regional node biopsy • Thickness 1-4 mm • Thickness < 1mm • Has <10% of nodal metastasis no biopsy • Ulceration, truncal location, and male gender, either alone or in combination consider biopsy to evaluate nodal metastasis • Thickness > 4mm • Has 65-70% distant metastasis no biopsy
Histological examination of nodes • Reverse transcriptase polymerase chain reaction (RT-PCR) assaydetects of tyrosinase messenger RNA, a melanocyte-specific marker, in lymph nodes with metastasis • Immunohistochemistry techniques
Staging • Depth of invasion • Regional nodal metastasis • Distance metastasis
LDH Prognostic indicator for distant metastasis in stage IV
Cutaneous excision Recommendations from Academy of Dermatology • A margin of 0.5 cm of normal skin is recommended for in situ melanomas. • A 1 cm margin is recommended for melanomas <2 mm thick • A 2 cm margin is recommended for melanomas 2 mm thick
Other recommendations • Surgical margin of 3 cm for T3 (2.1 to 4.0 mm) or T4 (>4 mm) primary tumors • No correlation between thickness > 4mm and surgical margin (Heaton et al. Ann Surg Oncol 1998) • In >4mm thickness, outcome is probably based more on regional and distant metastasis
Head and neck melanomas • Face and scalp – high recurrence rate • Complex regional node drainage • Parotid and cervical lymphatics are common sites of spread • Parotid node dissection – risk of CN VII injury • Limited skin – skin graft • Post-op adjuvant radiation for unsatisfactory margin and desmoplastic neurotropic melanomas
Subungual melanoma • Fingers • Amputation DIP • Cutaneous excision and skin graft for proximal lesions • Toes • Amputation at MTP
Plantar melanoma Cutaneous excision with skin graft due to lack of surplus skin
Positive sentinel nodes Regional lymph node dissection
Noncerebral metastatic melanoma • Cytotoxic chemotherapy • Immunotherapy such as interferon • Pallative • Radiation • Surgery
Cerebral metastatic melanoma • Surgery • Whole brain radiation therapy • And/or stereotactic radiosurgery