Download
1 / 39
410 likes | 727 Views
Melanoma, the sixth most common cancer, is highly lethal despite accounting for only 1% of skin cancers. This article discusses risk factors, clinical prediction rules, growth patterns, diagnostic tests, and treatment options for melanoma. It includes details on different types of melanoma, diagnostic tests like excisional biopsy, and guidelines for surgical margins based on tumor thickness. The text also covers the management of head and neck, subungual, and plantar melanomas, as well as treatments for positive sentinel nodes and metastatic melanoma.

E N D
Melanoma Hai Ho, M.D. Department of Family Practice
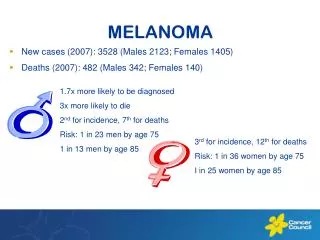
Epidemiology • Sixth most common cancer • Incidence increases from 1/1500 in 1930 to 1/75 in 2000 • 1% of skin cancer but account for 60% of skin cancer death
Risk factors? • Sun exposure • Intermittent intense exposure • Childhood • UVB > UVA – higher incidence near equator • Tanning bed
Clinical prediction rule American Cancer Society’s ABCDE
D Melanoma could occur in lesions less than 6 mm
E Elevation or Enlargement by patient report
Sensitivity of ABCDE rule If melanoma truly exists, the rule will detect it 92-97% (average 93%) of the time, when one criterion is met
Caution • If none of the criteria is met, 99.8% chance that the lesion is not a melanoma (high negative predictive value) • May miss amelanotic melanomas and melanomas changing in size
Growth patterns • Radial growth • Lasts for months to years • Growth and regression due to restraint by immunologic system • Horizontal and vertical growth • More poorly differentiated • Produce nodule or mass
Superficial spreading melanoma White = regression • 50% of melanoma cases • Common in middle age • Radial spread and regression
Nodular melanoma • 20-25% of melanoma cases • Common in 5-6th decade • Vertical growth and no horizontal growth phase
Lentigo maligna melanoma Lentigo maligna Lentigo maligna melanoma • 15% of melanoma cases • Elderly – 6-7th decade • Lentigo maligna • Horizontal growth phase for years • Bizarre shapes from years of growth and regression • Transform to lentigo maligna melanoma
Acral-lentigious melanoma • 10% of melanoma cases • In palms, soles, terminal phalanges, and mucous membrane • Growth phase similar to lentigo maligna and lentigo maligna melanoma • Aggressive tumor and early metastasis
Excisional biopsy Preferred method – deepest level of penetration for staging
Punch biopsy Stretch the skin perpendicular to the skin line Subcutaneous fats Wound <4mm may not be sutured
Shaving Never because prognosis and treatment are based on the level and depth of invasion
Pathology • Depth of invasion • Growth pattern (nodular, superficial spreading, etc.) • Margin status • Presence or absence of ulceration
Depth of invasion • Breslow • Measure the actual thickness • More reproducible and accurate in determining prognosis • Clark • Report by anatomical site • Significant if tumor ≥ 1mm
Indications for regional node biopsy • Thickness 1-4 mm • Thickness < 1mm • Has <10% of nodal metastasis no biopsy • Ulceration, truncal location, and male gender, either alone or in combination consider biopsy to evaluate nodal metastasis • Thickness > 4mm • Has 65-70% distant metastasis no biopsy
Histological examination of nodes • Reverse transcriptase polymerase chain reaction (RT-PCR) assaydetects of tyrosinase messenger RNA, a melanocyte-specific marker, in lymph nodes with metastasis • Immunohistochemistry techniques
Staging • Depth of invasion • Regional nodal metastasis • Distance metastasis
LDH Prognostic indicator for distant metastasis in stage IV
Cutaneous excision Recommendations from Academy of Dermatology • A margin of 0.5 cm of normal skin is recommended for in situ melanomas. • A 1 cm margin is recommended for melanomas <2 mm thick • A 2 cm margin is recommended for melanomas 2 mm thick
Other recommendations • Surgical margin of 3 cm for T3 (2.1 to 4.0 mm) or T4 (>4 mm) primary tumors • No correlation between thickness > 4mm and surgical margin (Heaton et al. Ann Surg Oncol 1998) • In >4mm thickness, outcome is probably based more on regional and distant metastasis
Head and neck melanomas • Face and scalp – high recurrence rate • Complex regional node drainage • Parotid and cervical lymphatics are common sites of spread • Parotid node dissection – risk of CN VII injury • Limited skin – skin graft • Post-op adjuvant radiation for unsatisfactory margin and desmoplastic neurotropic melanomas
Subungual melanoma • Fingers • Amputation DIP • Cutaneous excision and skin graft for proximal lesions • Toes • Amputation at MTP
Plantar melanoma Cutaneous excision with skin graft due to lack of surplus skin
Positive sentinel nodes Regional lymph node dissection
Noncerebral metastatic melanoma • Cytotoxic chemotherapy • Immunotherapy such as interferon • Pallative • Radiation • Surgery
Cerebral metastatic melanoma • Surgery • Whole brain radiation therapy • And/or stereotactic radiosurgery