Download
1 / 84
880 likes | 1.25k Views
Fractures & Dislocations of the Upper Limb. Dr Munir Saadeddin, FRCSE. Upper Limb include. Clavicle Scapula Shoulder Joint Humerus Elbow Joint Forearm Bones Wrist Joint Scaphoid Bone. Mechanism of Injuries of the Upper Limb. Mostly Indirect

E N D
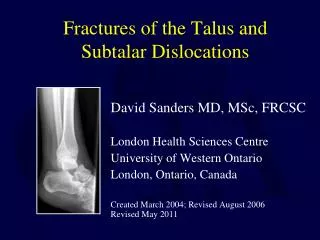
Fractures & Dislocations of the Upper Limb Dr Munir Saadeddin, FRCSE
Upper Limb include • Clavicle • Scapula • Shoulder Joint • Humerus • Elbow Joint • Forearm Bones • Wrist Joint • Scaphoid Bone
Mechanism of Injuries of the Upper Limb • Mostly Indirect • Commonly described as “ a fall on outstretched hand “ • Type of injury depends on position of the upper limb at the time of impact : Flexed, Extended, adducted, abducted, pronated or supinated
Splintage & Elevation in Upper Limb • The Hand has to be Higher than the Elbow • Simplest splint is the tri-angular splint which can be made of any piece of cloth • Commonest splint used is the Collar & cuff splint • Strapping the upper limb to the trunk is one method of Immobilisation of shoulder and humerus
Fractures of the Clavicle • A common injury in all ages • Most fractures are in the Middle third • Usually it is the result of Indirect injury • Direct injuries are more serious ( possible injury to neuro vascular structures ) • In children it may be a Green stick fracture • Fracture site can be identified easily because clavicle is a subcutaneous bone
? Fracture of the clavicle • A child with sudden painful swelling over left clavicle • History of a fall injury few days ago • The swelling is over mid clavicle and is tender • Initial x rays do not show a fracture • The Answer is to repeat the X ray two weeks later
Fracture of the clavicle in Adults • Usually displaced with deformity • May be comminuted • mostly heal with a degree of Mal-Union • Delayed union or Non union are less common • Usually is treated conservatively • Open reduction gives satisfactory alignment but results in unsightly scar
Figure of Eight bandage • It is the common way for treating fractures of clavicle conservatively • Simple to apply in Emergency room • It helps to reduce overlap of fracture ends • It should not be applied very tight or it may compress the neuro vascular structures at axilla
Union of Fracture of the clavicle • Early union occurs in 1-2 weeks in children • In adults early union occurs in 3 weeks , union in 6 weeks and consolidation in 12 weeks • Callus formation can be visible and palpable • Mal united overlap of fracture can be treated by trimming some bone after union of fracture • Non Union is treated by compression Plating and bone grafting
Dislocation of the Shoulder • Mostly Anterior> 95 % of dislocations • Posterior Dislocation occurs < 5 % • True Inferior dislocation ( Luxato Inferno ) occurs < 1% • Habitual Non traumatic dislocation may present as Posterior dislocation or Multi directional dislocation due to ligament laxity and is Painless
Mechanism of anterior shoulder dislocation • Usually Indirect fall on Abducted and extended shoulder • May be direct when there is a blow on the shoulder from behind
Anterior Shoulder dislocation • Usually also inferior • There is damage ( Overstretching ) to the shoulder capsule and subscapularis muscle • Commonly there is avulsion to the antero inferior part of the Glenoid labrum with adjacent periosteom on the neck of scapula = Bankart’s Lesion
Clinical Picture • Patient is in pain • Holds the injured limb with other hand close to the trunk • The shoulder is abducted and the elbow is kept flexed • There is loss of the normal contour of the shoulder
Clinical Picture • Loss of the contour of the shoulder may appear as a step • Anterior bulge of head of humerus may be visible or palpable • A gap can be palpated above the dislocated head of the humerus
Associated injuries of anterior Shoulder Dislocation • Injury to the neuro vascular bundle in axilla ( rare ) • Injury ofthe Axillary or Circumflex Nerve ( Usually stretching leading to temporary neuropraxia ) • Associated fracture
Axillary or Circumflex Nerve Injury • It is a branch from posterior cord of Brachial plexus • It hooks close round neck of humerus from posterior to anterior • It pierces the deep surface of deltoid and supply it and the part of skin over it
Management Of Anterior Shoulder dislocation • Is an Emergency • It should be reduced in less than 24hours or there may be Avascular Necrosis of head of humerus • Following reduction the shoulder should be immobilised strapped to the trunk for 3-4 weeks and rested in a collar and cuff
Methods of Reduction of anterior shoulder Dislocation • Hippocrates Method ( A form of anesthesia or pain abolishing is required ) • Stimpson’s technique ( some sedation and analgesia are used but No anesthesia is required ) • Kocher’s technique is the method used in hospitals under general anesthesia and muscle relaxation
Complications of anterior Shoulder Dislocation : Early • Neuro vascular injury ( rare ) • Axillary or Circumflex nerve injury • Associated Fracture of neck of humerus or greater or lesser tuberosities
Complications of anterior shoulder Dislocation : Late • Avascular necrosis of the head of the Humerus ( may be delayed up to 2 years and only following delayed reduction ) • Heterotopic calcification ( used to be called Myositis Ossificans ) • Recurrent dislocation
Fractures of The Humerus • Proximal Humerus (includes surgical and anatomical neck ) • Shaft of Humerus • Distal humerus ( includes Supra Condylar fracture in children )
Fractures Shaft of the Humerus • Commonly Indirect injury • Indirect injury results in Spiral or Oblique fractures • Direct injuries results in transverse or comminuted ( Butterfly ) fracture • May be associated with Radial Nerve injury
Radial Nerve Injury • Results in Drop Wrist • Associated with fracturehumerus in up to 12% of fractures • 2/3 ( 8%) of Radial injury are Neuropraxia • 1/3 ( 4%) are nerve lacerations or transection
Management of Radial Nerve Injury • When present in open fractures ; immediate exploration and ± repair • In closed injuries treated conservatively ; initial management is doing Nerve Conduction Studies ( NCS ) and Electromyography ( EMG ) and awaiting for spontaneous recovery
Management of Radial Nerve injury • Recovery usually starts after few days but may take up to 9 months for full recovery • If No spontaneous recovery occurs in 12 weeks confirmed by NCS and EMG ;then exploration of the nerve should be carried out
Management of Fracture Shaft of the Humerus • Preferably Conservative • Closed Reduction in upright position followed by application of U shaped Slap of POP or Cylinder cast • Few weeks later or initially in stable fractures Functional Brace may be used
Indications for ORIF Fracture Shaft of Humerus • Failure to reduce fracture conservatively • Bilateral humeral fractures • Open fracture with radial nerve Injury • Unconscious patient • Delayed-Union, Non-Union and Mal-Union