Download
1 / 50
1.68k likes | 5.96k Views
Immune Thrombocytopenic Purpura. Kenny Aristide, Pharm.D. PGY-1 Pharmacy Resident Thursday, October 4, 2012. Pharmacist Objectives. Discuss the etiologies associated with immune thrombocytopenic purpura Describe the pathophysiologic processes of immune thrombocytopenic purpura

E N D
Immune Thrombocytopenic Purpura Kenny Aristide, Pharm.D. PGY-1 Pharmacy Resident Thursday, October 4, 2012
Pharmacist Objectives Discuss the etiologies associated with immune thrombocytopenic purpura Describe the pathophysiologic processes of immune thrombocytopenic purpura Define the diagnostic criteria for immune thrombocytopenic purpura Differentiate between the various pharmacologic agents utilized to treat immune thrombocytopenic purpura Critique the clinical trials of the pharmacologic agents utilized to treat immune thrombocytopenic purpura
Pharmacy Technician Objectives Identify patients with immune thrombocytopenic purpura Identify the pharmacologic agents utilized to treat immune thrombocytopenic purpura List the generic names of the medications that are utilized to treat immune thrombocytopenic purpura
Definition: Immune (Idiopathic) Thrombocytopenic Purpura (ITP) • Disorder of exclusion • Clinical syndrome of diverse disorders1 • Differentiated from non-autoimmune etiologies of thrombocytopenia2 • Stasi R. Semin Thromb Hemost.2012;38(5):454-62. • Cuker A. et al. Hematology. 2010;33:377-383.
Epidemiology of ITP • Incidence • Children: 5 per 100,000 • Adults: 2 per 100,000 • Gender • Children and elderly: affects both equally • Adults: more common in females • Age • Prevalence peaks in childhood • Peak age 2 – 5 Lakshmanan S, Cuker A. J Thromb Haemost. 2012.
Epidemiology of ITP: Age and sex distribution Beutler et al. Williams Hematology. 1995.
Etiology of ITP • Often following infection (viral or bacterial) • Postulated theories • Molecular Mimicry • Viral infection (HIV, HCV) • H. pylori infection • Autoantibodies Autoimmunity Chong BH. J Thromb Haemost. 2009;7(2):319-21.
Classification of ITP • Primary ITP • Idiopathic – no known etiology • No clinically evident secondary form • Secondary ITP • Associated with infections, immunizations/vaccines Stasi R. Semin Thromb Hemost. 2012;38(5):454-62.
Classification of ITP • Secondary ITP • Antiphospholipid syndrome • Autoimmune thrombocytopenia (e.g., Evans syndrome) • Common variable immune deficiency • Infection with cytomegalovirus, Helicobacter pylori, hepatitis C (HCV), human immunodeficiency virus (HIV), varicella zoster • Lymphoproliferative disorders • Bone marrow transplantation side effect • Vaccination side effect (i.e. MMR) • Systemic lupus erythematosus Stasi R. Semin Thromb Hemost. 2012;38(5):454-62.
Classification of ITP Estimated Prevalence of Secondary ITP in the US SLE 5% APS 2% CVID 1% CLL 2% Primary80% Evan’s 2% ALPS, post-tx 1% HIV 1% Hep C 2% H. pylori 1% Postvaccine 1% Misc systemic infection 2% Adapted from Cines DB, et al. Blood. 2009;113:6511-6521.
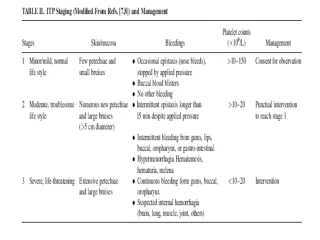
Classification of ITP:Disease phases • Newly diagnosed ITP • Less than 3 months • Persistent ITP • 3 – 12 months • Chronic ITP • Greater than 12 months • Refractory ITP • Treatment failure of splenectomy
Pathophysiology of ITP • Harrington-Hollingsworth experiment1 • Established the autoimmune nature of ITP • Autoimmune response2 • IgG mediated response to platelet glycoproteins (GP IIb/IIIa and Ib/IX) • Platelet destruction + Decreased platelet production • Stasi R. Semin Thromb Hemost. 2012;38(5):454-62. • Chong BH. J Thromb Haemost. 2009;7(2):319-21
Pathophysiology of ITP • Cines DB, et al. N Engl J Med. 2002;346:995-1008.
Two Processes Involved in Immune Thromcytopenic Purpura Antibody Antibody Platelets Bone marrow where platelets are produced & Increased platelet destruction Inadequate platelet production
Assessment Question What is the most commonly identified antigenic target of the ITP autoantibodies? • VH1 • GP IIb/IIIa • ITP IIIa • GP IVc/IX
Clinical Presentation of ITP • Bleeding • most important clinical manifestation of ITP • Petechiae • Ecchymoses • Epistaxis • Gingival bleeding • Menorrhagia • Major hemorrhage (GI bleed, CNS bleed) – rare • Disabling fatigue • Withdrawal from professional and social activities
Clinical Presentation of ITP Purpura and Petechiae. Available at: http://www.nhlbi.nih.gov/health/health-topics/images/itp_photo.jpg
Diagnosis of ITP • Platelet count • Less than 100 x 109/L (rather than 150 x 109/L) • Medical History • Response to therapy • Peripheral Smear • Physical Exam • Bone marrow aspiration and biopsy • Not routinely done • Antiplatelet Antibody Testing
Assessment Question In order to make the diagnosis of ITP, a bone marrow biopsy must be performed. • True • False
Indications for Treatment American Society of Hematology (ASH) suggests: • Platelet counts > 30 x 109/L usually have few or no symptoms and require no treatment • Avoid treatment in patients with mild, asymptomatic disease • Platelet counts < 30 x 109/L have treatment recommendations based on the presence and severity of associated bleeding symptoms • Hospitalization and emergent treatment is indicated if: • Severe bleeding occurs, regardless of platelet count • Platelet count < 20 x 109/L and signs/symptoms of mucocutaneous bleeding is present
Goals of Treatment • Obtain a hemostatic platelet count to prevent bleeding • Individualized to the patient • Minimizing toxicity associated with treatment • Induce long-term remission
ITP Treatment Options • 1st line • Corticosteroids • Intravenous immunoglobulins (IVIG) • 2nd Line • Splenecotomy • Thrombopoietin Receptor Agonists • Rituximab • 3rd Line • Other immunosuppressive agents
ITP Treatment Options: Corticosteroids • Prednisone • Mechanism of Action: • Impair clearance of platelets in the bone marrow and peripherally • Reduce antibody production • Dose: • 1 – 2 mg/kg/day PO as single or divided doses • Usually responds within 2 - 3 weeks • Response rate: 50 – 75% • Taper over 4 – 6 weeks following platelet response • Side effects: numerous
Assessment Question All of the following are side effects of corticosteriods except: • Bone density loss • Hypertension • Weight loss • Muscle weakness
ITP Treatment Options: IVIG • IVIG • Mechanism of action: • Undefined and potentially multifactorial • Dose: • Variable regimen • Standard dose: 1 g/kg/day x 1 – 2 days • Side effects: - hypersensitivity -headache - renal failure -nausea/vomiting - alloimmune hemolysis -pulmonary edema George JN. Am J Hematol. 2012;87 Suppl 1:S12-5.
ITP Treatment Options • 1st line • Corticosteroids • IVIG • Anti-D immunoglobulins • 2nd Line • Splenecotomy • Rituximab • Thrombopoietin Receptor Agonists • 3rd Line • Other immunosuppressive agents
ITP Treatment Options:Splenectomy • Splenectomy • Mechanism of action: • Removes a primary site of platelet destruction and increases platelet count • Possible site of autoantibody production • Side effects: increase risk of infection, thrombosis, pulmonary hypertension • Vaccination recommended • HIB, pneumococcal, and meningococcal George JN. Am J Hematol. 2012;87 Suppl 1:S12-5.
Assessment Question Which of the following is a recommended vaccination patients should receive following splenecotomy? • Hepatitis C • Hepatitis B • Pneumovax • Tdap
Rituximab Anti-CD20 Antibody
ITP Treatment Options:Rituximab • Rituximab (Rituxan®) • Mechanism of action: • Hypothesis-driven use • B-cell depletion: ↓ antiplatelet antibodies • Dose: • Most effective dose/schedule not known, not FDA-approved for ITP • Usual dosage: 375 mg/m2 IV once weekly x 4 weeks • Response rate: • 40% at 1 year • 20 – 25% at 5 years • Side effects: -Infusion reaction - Tumor lysis syndrome -Pulmonary toxicity - Hepatitis B reactivation • Rituxan [package insert]. San Francisco, CA: Genentech, Inc.; 2012. • Lakshmanan S, Cuker A. J Thromb Haemost. 2012.
TPO Receptor Agonists • Romiplostim (Nplate®) • Mechanism of action: • Analog of thrombopoietin which increases the production of platelets • Dose: 1 – 10 mcg/kg SubQ weekly • Increase dose by 1 mcg/kg qweek to effect (Plts ≥ 50 x 109/L) • Side effects: • Headache - Paresthesia • Myelodysplastic Syndrome - Mylagia • Insomnia - Pain in extremity • Monitor: CBC with differential and platelets continually Nplate [package insert]. Thousand Oaks, CA: Amgen, Inc.; 2011.
TPO Receptor Agonists • Eltrombopag (Promacta®, Revolade®) • Mechanism of Action: • induces megakaryocyte proliferation and differentiation from bone marrow progenitor cells. • Dose: 12.5-75 mg PO daily • Reduce dosage in patients with East Asian ancestry (25 mg once daily initially) • Side effects: - Myalgia - Paresthesia - Hepatotoxicity (BBW) • Monitor: • LFTs, CBCs, and platelets Promacta [package insert]. Research Triangle Park, NC: GlaxoSmithKline; 2011.
Romiplostim vs. Standard of Care (SOC) in Patients with ITP Kuter et. al. NEJM. 2010:1889-1899
Romiplostim vs. Standard of Care (SOC) in Patients with ITP Kuter et. al. NEJM. 2010:1889-1899
Assessment Question What type of bias is the most closely associated with an open-label study design? • Participant bias • Recall or memory bias • Compliance bias • Selection bias
Eltrombopag for management of chronic immune thrombocytopenia (RAISE): 6 month, randomized, phase III study Cheng G et al. Lancet. Jan 29 2011;377(9763):393-402.
Eltrombopag for management of chronic immune thrombocytopenia (RAISE): 6 month, randomized, phase III study Results Cheng G et al. Lancet. Jan 29 2011;377(9763):393-402.
Eltrombopag for management of chronic immune thrombocytopenia (RAISE): 6 month, randomized, phase III study Results Cheng G et al. Lancet. Jan 29 2011;377(9763):393-402.
Conclusion • ITP is an disorder of exclusion • Multiple therapies available • may be needed to induce remission • Goal of treatment = prevention of complications
Comparison of TPO Receptor Agonists:Romiplostim Vs. Eltrombopag *AWP = Average Wholesale Price Murray L, ed. 2009 Red Book. Montvale, NJ: Thomson PDR; 2009.
Case Subjective: 60 yo female who notice sudden appearance of multiple petechiae on her extremities and mild epistaxis. She had no other symptoms. PMH: Hep C related liver cirrhosis (status post liver transplant in 2010) and Meds: Cyclosporine A, mycophenolate and a low dose prednisone. Objective: Platelet count: 20 x 109/L Bone marrow biopsy was suggestive with ITP, showing an activated megakaryocytopoiesis and normal reticulin distribution.
Case Assessment: According to the AHS guidelines, pt received standard therapy (prednisone 1 mg/kg/day) obtaining only a transient response. Plan: Her physician would like treat the patient with one of the new TPO receptor agonists and he turns to you to recommend one of the two agents available on formulary, Romiplostim or Eltrombopag. Based on the data presented, which of the two agents do you recommend?
References • Stasi R. Immune thrombocytopenia: pathophysiologic and clinical update. Semin Thromb Hemost. 2012;38(5):454-62. • Cuker A., Cines DB. Immune Thrombocytopenia. Hematology. 2010;33:377-383. • Lakshmanan S, Cuker A. Contemporary Management of Primary Immune Thrombocytopenia (ITP) in Adults. J Thromb Haemost. 2012. • George JN. Sequence of treatments for adults with primary immune thrombocytopenia. Am J Hematol. 2012;87 Suppl 1:S12-5. • Chong BH. Primary immune thrombocytopenia: understanding pathogenesis is the key to better treatments. J Thromb Haemost. 2009;7(2):319-21. • Cines DB, Blanchette VS. Immune Thrombocytopenic Purpura. N Engl J Med. 2002;346:995-1008 • Beutler E, Lichtman, MA, Coller BS et al. Williams Hematology, 5th ed. McGraw-Hill, New York, 1995. • Nplate [package insert]. Thousand Oaks, CA: Amgen, Inc.; 2011. • Rituxan [package insert]. San Francisco, CA: Genentech, Inc.; 2012. • Promacta [package insert]. Research Triangle Park, NC: GlaxoSmithKline; 2011. • Kuter DJ, Rummel M, Boccia R. et. al. Romiplostim or standard of care in patients with immune thrombocytopenia. N Eng J Med. 2010;363:1889-99. • Cheng G, Saleh MN, Marcher C, et al. Eltrombopag for management of chronic immune thrombocytopenia (RAISE): a 6-month, randomised, phase 3 study. Lancet. Jan 29 2011;377(9763):393-402.