Download
1 / 85
860 likes | 946 Views
Idiopathic Thrombocytopenic Purpura. הצגת מקרה. נ.ד ילדה בת 10 שנים שהתקבלה עקב פריחה פטכיאלית בגוף, לציין שסבלה מדלקת גרון כעשרה ימים טרם קבלתה. בבדיקה בקבלה : אכימוזות ופטכיות מפושטות על פני הגוף, שאר הבדיקה תקינה ללא הגדלת בלוטות לימפה וללא אורגנומגליה.

E N D
הצגת מקרה • נ.ד ילדה בת 10 שנים שהתקבלה עקב פריחה פטכיאלית בגוף, לציין שסבלה מדלקת גרון כעשרה ימים טרם קבלתה. • בבדיקה בקבלה : אכימוזות ופטכיות מפושטות על פני הגוף, שאר הבדיקה תקינה ללא הגדלת בלוטות לימפה וללא אורגנומגליה. • בדיקות מעבדה : מס' טסיות – 10.600 ללא דיכוי של שאר השורות. • הושלמה בדיקת פונדוסים ושתן לכללית – תקינים.
המשך... • לאור ההתייצגות הקלינית והמעבדתית סוכמה שקרוב לוודאי ITP. • הילדה שוחררה להמשך מעקב אמבולטורי ללא טיפול תרופתי. • כעבור שנה מהאבחנה עדיין מס‘ טסיות נמוך סביב 9700 , טופלה בקורס של IVIGשגרם לתגובה קצרת טווח, שבהמשך הופסק לאור הופעת כאבי ראש חזקים.
המשך.... • נשלחו נוגדנים נגד טסיות לרמב"ם ??? • לאור תמונה של Chronic ITPנשלח בירור שכלל : ANA Anti ds DNA , Anti cardiolipin,
המשך... • כעבור שנתיים מהאבחנה לאור טרומבוציטופניה סביב 7000 הוחלט להתחיל טיפול בסטירואידים (פרדנזון של 60 מ"ג ליום). • טרם התחלת הסטירואידים בוצעה בדיקת לשד עצם שהראתה ריבוי מגקריוציטים . • לאחר התחלת סטירואידים היתה עלייה במספר הטסיות ל 40.000 . • הבעייתיות היתה תלות מלאה בטיפול ותגובה שחלפה עם הורדת המינון.
המשך.... • בשנת 2004 היה ניסיון עם Rituximabללא הטבה (טסיות נשארו סביב 7000 ). • ב 07.2004 הועלתה אפשרות של Splenectomy • מאז 07.2001 טסיות סביב 5000 – 20.000 • ס"ד אחרונה ב 04.2006 – מספר טסיות סביב 12.000
ITP 100 cases per 1 milion persons per year. About half of these cases occur in children. Primary vs Secondary . Acute vs Chronic ( >6 months).
The etiology is still unknown and the pathogenesis is complex and possibly depends on disturbed antigen presentation, T cell activation and signaling, disregulated B cell stimulation and antibodies, unbalanced activation / suppression of complement.
Affected children are young (peak age ~ 5yrs) and previously healthy, and they typically present with the sudden onset of petechiae or purpura a few days or weeks after an infectious illness. Boys and girls are equally affected.
In more than 70% of children, the illness resolves within six months, irrespective of whether they receive therapy. By contrast, ITP in adults is generally chronic.
The bone marrow in patients with ITP contains normal or increased numbers of megakaryocytes.
Pathophysiology ITP is mediated by IgG autoantibodies. Glycoprotein IIb/IIa, Ib/Ix, Ia/IIa, IV and V ... Accelerated clearance through Fcү receptors that are expressed by tissue macrophages (spleen & liver).
Genetics Monozygotic twins. An increased prevalence of HLA-DRw2 and DRB1*0410 alleles. HLA-DR4 and DRB1*0410 alleles have been associated with unfavorable and favorable response to corticosteroids, respectively.
Diagnosis The diagnosis of ITP remains one of exclusion. Secondary forms of the disease occur in association with SLE, the antiphospholipid syndrome, immunodeficiency states (IgA deficiency and common variable hypogammaglobulinemia), Lymphoproliferative disorders (CLL, Large granular lymphocytic leukemia, and lymphoma), infection with HIV and hepatitis c virus, and therapy with drugs such as heparin and quinidine.
The guidelines of the American Society of Hematology state that a bone marrow examination is not required in adults younger than 60 yrs of age if the presentation is typical but is appropriate before splenectomy is performed.
Marrow examination is necessary in the presence of atypical features (e.g., those with additional cytopenias, protracted fever, bone or joint pain, unexplained macrocytosis ), or in patients who do not have a brisk or robust response to therapy.
There is consensus, that bone marrow examination is not necessary in children if management involves observation or IVIG. Although it is not mandatory, many pediatric hematologists recommend that an aspiration be performed before starting corticosteroids to rule out the rare case of acute leukemia.
The direct assay for the measurement of platelet-bound AB’s has an estimated sensitivity of 49-66%, an estimated specificity of 78-92%, and an estimated PPV of 80-83%.
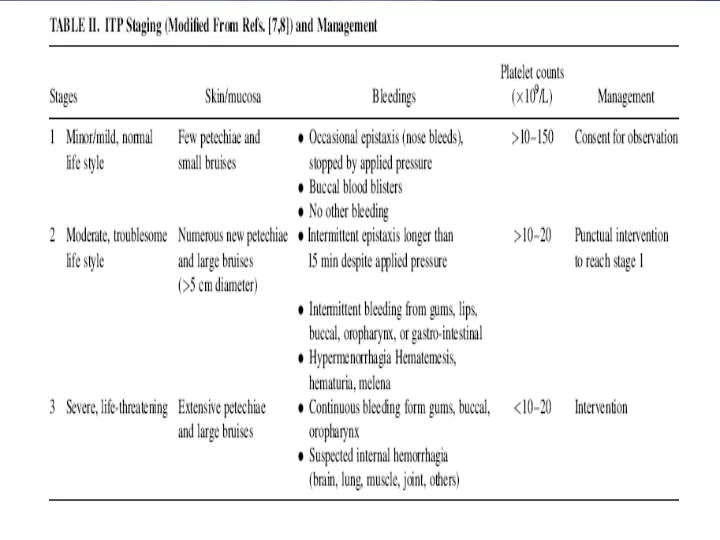
The decision to treat ITP is based on theplatelet count, the degree of bleeding, and the patient’s lifestyle .
Management The incidence of intracranial hemorrhageis ~ between 0.2-1%. Almost all intracranial hemorrhages occur at platelet counts below 20.000/mm3, and generally below 10.000/mm3. Risk factors : head trauma and exposure to antiplatelet drugs.
Most intracranial hemorrhagrs occur within four weeks after presentation with ITP, often within the first week.
Most children with typical acute ITP recover completely within a few weeks without treatment and that there is no proof that therapy prevents intracranial hemorrhage.
ITP in many children – certainly those without hemorrhage –is managed on an outpatient basis with minimal investigation, short-term therapy in select cases, and the avoidance of activities that predispose the patient to trauma and of medications that impair platelet function.
American Society of Hematology (ASH) recommends drug therapy for children with platelet counts of less than 10.000/mm3 with little or no purpura.
The UK guidelines state : only patients who experience significant mucous membrane bleeding receive treatment.
Treatment Watch & Wait strategy. Corticosteroids (high, standard or low dose). IVIG (high or low dose, 2 day or 1 day). IV anti-D immunoglobulin in Rh(D) positive patients (high or low dose).
Randomized clinical trials have demonstrated that therapy with IVIG shortens the duration of severe thrombocytopenia ( platelet < 20.000 /mm3) . Adverse reactions : headache, fever, nausea, and aseptic meningitis. The response to IVIG is more rapid than the response to IV anti-D. The average decrease in the hemoglobin level is 1.3 g per deciliter, and intravascular hemolysis is rare.
Urgent treatment Neurologic symptoms, internal bleeding, or emergency surgery demands immediate intervention. IV.Methylprednisone (30 mg/Kg/d; max 1 gr/d for 2-3 days) / 20-30min + IVIG (1 gr/kg/d for 2-3 days) + infusion of platelets that is 2-3 times the usual amount infused; Vincristine may be considered.
Splenctomy should be considered if it has not yet been performed. Plasmapheresis is of limited benefit. Antifibrinolytic therapy (e.g. Aminocaproic acid) may reduce mucosal bleeding, and recombinant factor VIIa should be considered.
Management of first relapse Approximately 25% of children with ITP have a relapse after initial treatment. One third of children have spontaneous remission and only 5% still have severe thrombocytopenic requiring therapy one year after diagnosis.
Guidelines from the American Society of Hematology recommended that splenctomy be considered for children who have had ITP for at least one year with symptomatic, severe thrombocytopenia. In children, the rate of complete remission after splenectomy is 70-80%. Bacterial sepsis ( ~ 3%) !!!!
Chronic refractory ITP Achallenge is posed by the occasional symptomatic child in whom splenectomy fails or is containdicated and in whom the platelet count cannot be sustained with acceptable doses of corticosteroids, anti-D immune globulin.
American Soceity of Hematology guidelines recommend treatment for such children if they have symptomatic thrombocytopenia and platelet counts of less than 30.000/mm3. No regimen is universally effective. Vincristine, azathioprine, cyclophosphamide or cyclosporine.
Childhood ITP in the nordic countriesActa paediatrica 2005;94 A prospective registration 1998 – 2000. Ninety eight paediatric departments. 506 children with newly ITP aged 0-14 yr and at least one platelet count <30.000 . 423 of the children followed for 6 months. The platelet count < 10.000 in 58%. Chronic ITP developed in 25% : thrombocytopenia < 150.000 persisting after 6 months.
Cont’d Most cases in the winter months from October to March. About 57.7% of the children have various infections in the 4 wk preceding diagnosis. The majority had viral URI, flu-like diseases or unspecified fever. Some patients developed ITP following a bacterial infection like sinusitis, otitis media or tonsillitis.
Cont’d In 6.9% cases, ITP occured after vaccinations, particularly the MMR vaccination (DTP, Oral polio, Hepatitis A & B).
Cont’d Factors associated with chronic ITP : Insidious onset of symptoms. A bsence of preceding infection and/or vaccination. Age 8-14 yrs. Female gender.
Treatment soon after diagnosis did not appear to influence the risk of developing chronic disease.
The frequency of mucosal bleeding was related to the initial platelet count (<15000). 3/15 patients with severe haemorrhage had platelet count between 16 – 24.000 .
Corticosteroids versus IVIG forthetreatment of acute ITP in childrenJ Pediatr 2005; 147 A systematic review and meta-analysis of randomized controlled trials comparing corticosteroids with IVIG. 10 studies were included. The primary outcome was the number of patients with a platelet count >20.000, 48 hrs after treatment initiation.