Download
1 / 8
120 likes | 389 Views
Strongyloides stercoralis. History : Observed in 1876 by Normand in the intestines of French soldier in Cochin-China. Found mainly in moist tropical countries and temperate regions. Morphology:. Clinical manifestations : 1. Cutaneous reaction due to skin penetration ground itch

E N D
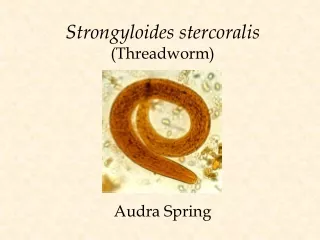
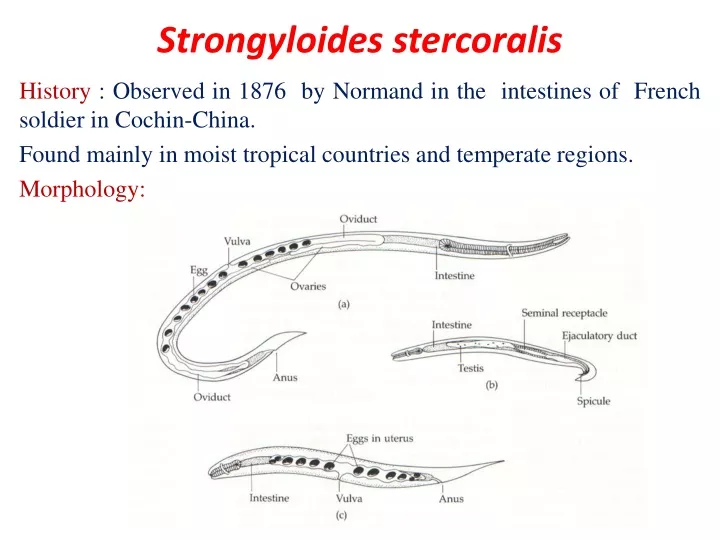
Strongyloidesstercoralis History : Observed in 1876 by Normand in the intestines of French soldier in Cochin-China. Found mainly in moist tropical countries and temperate regions. Morphology:
Clinical manifestations: 1. Cutaneous reaction due to skin penetration ground itch 2. Pulmonary symptoms (including Loeffler’s syndrome) can occur during 3. pulmonary migration of the filariform larvae. 4. Gastrointestinal symptoms include abdominal pain, vomiting, diarrhea, weight loss, malabsorption,. 5. Dermatologic manifestations include urticarial rashes in the perianal and perineal areas (larva migrans). • Autoinfection within the human host can lead to the (Hyperinfection Syndrome) or disseminated strongyloidiasis occurs in- • immunosuppressed patients, • neurologic(CNS), heart, lung , liver • complications and septicemia. • This syndrome is potentially fatal.
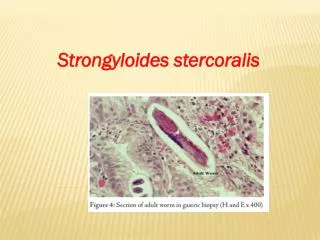
Laboratory Diagnosis • Direct stool smears (larvae) • Cultivation of stool. (Damp charcoal or Harada-Mori mediums). • Histological examination of duodenal or jejunal biopsy specimens obtained by endoscopy can demonstrateadult worms embedded in the mucosa. • Eosinophilia, is present in uncomplicated strongyloidiasis, but is lost in hyper infection • For population screening in endemic areas, an ELISA for IgG anfi-Strongyloides antibodies is effective.